

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Comparative Effectiveness Review Summary Guides for Clinicians [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2007-.
This publication is provided for historical reference only and the information may be out of date.

This guide summarizes clinical evidence about the effectiveness and safety of angioplasty and medical therapy for treating atherosclerotic renal artery stenosis (ARAS). This guide does not address how to choose among diagnostic strategies for evaluating suspected ARAS, and it does not discuss renal artery stenosis due to fibromuscular dysplasia.
Clinical Issue
Atherosclerosis causes 90 percent of all renal artery stenosis, the narrowing of one or both renal arteries. It can adversely affect blood pressure and kidney function. Among people with diffuse atherosclerotic vascular disease, as many as half develop ARAS. Medical therapy with antihypertensive drugs can reduce blood pressure in most people with ARAS. While medical therapy can lower the risk of cardiovascular events, it does not always prevent deterioration of kidney function. Historically, surgical repair of the blocked artery was the definitive treatment for ARAS, but newer procedures have largely supplanted surgery. Currently, the most common method of improving renal artery blood flow is percutaneous balloon angioplasty with stent placement.
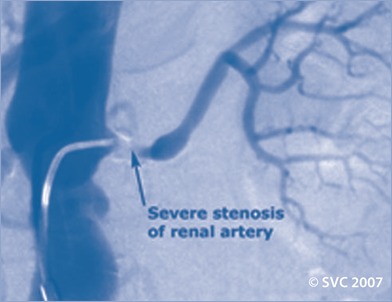
Arteriogram Showing Renal Artery Stenosis
Image reproduced by permission from the Society for Vascular Surgery. For more information visit www.VascularWeb.org.
Clinnical Bottom Line
Overall, there is insufficient evidence to determine whether angioplasty with stenting is a better treatment for ARAS than aggressive medical therapy alone.
- There is no difference in the long-term kidney function of people who have angioplasty compared with people who have medical therapy alone.LEVEL OF CONFIDENCE

- Both medical therapy and angioplasty lower blood pressure. Antihypertensive drugs can lower blood pressure 20 – 50 mm Hg systolic and 8 – 42 mm Hg diastolic. The combination of angioplasty and antihypertensive drugs typically lowers blood pressure 6 –32 mm Hg systolic and 0–17 mm Hg diastolic.LEVEL OF CONFIDENCE
- Attainment of blood pressure control is more likely after angioplasty than with medical therapy alone. However, the benefit of angioplasty may be limited to people with bilateral disease.LEVEL OF CONFIDENCE
- A small percentage of people who have had angio-plasty plus stent (4–18 percent) can discontinue blood pressure medications.LEVEL OF CONFIDENCE
Confidence Scale
The confidence ratings in this guide are derived from a systematic review of the literature. The level of confidence is based on the number and quality of individual studies, duration of followup, and consistency across studies.
HIGH
 Consistent results from at
least two high-quality studies with long-term followup.
Consistent results from at
least two high-quality studies with long-term followup.
MEDIUM
Findings are supported but are
from fewer than two high-quality studies or from high-quality studies that lack
long-term outcomes.
LOW
 Results may be inconsistent or
based on moderate to poor quality studies or studies of a population that may
have little direct relevance to the question.
Results may be inconsistent or
based on moderate to poor quality studies or studies of a population that may
have little direct relevance to the question.
Risks
There are not enough data to compare the risks of adverse events for ARAS treatments, and there is insufficient evidence to determine whether rates of death or cardiovascular events differ between treatments. However, there is some information about the risks of each treatment.
Medication Risks
- The most common side effects of antihypertensive drugs are dizziness, sexual problems, headache, and cough.
Angioplasty Risks
- About 1 percent of people who have angioplasty die within the first 30 days after the procedure.
- 10 – 21 percent of people who have angioplasty with stent placement have restenosis within 40 months.
Still Unknown
- There are not enough data to know whether individual characteristics (such as baseline health status, diagnostic test results, or type of medications used for hypertension) have an effect on ARAS treatment outcomes.
- We do not know how different types of blood pressure medications compare in treating ARAS.
- There is insufficient evidence to determine whether angioplasty reduces the number of antihypertensive medications required after the procedure.
- There is no research about how angioplasty and medical therapy compare in treating people who have acutely decompensating hemodynamic and kidney function.
On the Horizon
Results from the Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial, currently underway, will be reported in 2010. This large, multi-center trial will examine whether patients with ARAS who undergo angioplasty with stent placement followed by aggressive medical treatment of hypertension have different outcomes than patients treated with aggressive medical treatment of hypertension alone.
Resource for Patients
Renal Artery Stenosis Treatments: A Guide for Consumers is a companion to this Clinician’s Guide. It can help people talk with their health care professional about ARAS. It provides information about:
- Types of ARAS treatments.
- Benefits and risks of ARAS treatments.
- Research findings about ARAS treatments.
- Seeking advice from a health care professional.
For More Information
For electronic copies of the consumer’s guide, this clinician’s guide, and the full systematic review, visit this Web site: www.effectivehealthcare.ahrq.gov
For free print copies call: The AHRQ Publications Clearinghouse, (800) 358–9295
Consumer’s Guide, AHRQ Pub. No. 07-EHC004-2A
Clinician’s Guide, AHRQ Pub. No. 07-EHC004-3
Source
The source material for this guide is a systematic review of 56 studies. The review, Comparative Effectiveness of Management Strategies for Renal Artery Stenosis (2006), was prepared by Tufts-New England Medical Center Evidence-based Practice Center. The Agency for Healthcare Research and Quality (AHRQ) funded the systematic review and this guide.
This guide was prepared by Sandra Robinson, M.S.P.H., Elizabeth Eckstrom, M.D., and David Hickam, M.D. of the Eisenberg Center at Oregon Health & Science University. They developed this guide using feedback from clinicians who reviewed preliminary drafts.
- Review Atherosclerotic renal artery stenosis--diagnosis and treatment.[Mayo Clin Proc. 2011]Review Atherosclerotic renal artery stenosis--diagnosis and treatment.Lao D, Parasher PS, Cho KC, Yeghiazarians Y. Mayo Clin Proc. 2011 Jul; 86(7):649-57.
- Outcomes of Hypertensive Patients with Renal Fibromuscular Dysplasia Compared with Patients with Concomitant Atherosclerotic Renal Artery Stenosis following Endovascular Therapy.[J Vasc Interv Radiol. 2015]Outcomes of Hypertensive Patients with Renal Fibromuscular Dysplasia Compared with Patients with Concomitant Atherosclerotic Renal Artery Stenosis following Endovascular Therapy.Jenkins TL, Baker MG, Baheti AR, Sharma AM, Patrie JT, Angle JF, Matsumoto AH. J Vasc Interv Radiol. 2015 May; 26(5):625-33; quiz 634.
- Review Diagnosis and therapy of atheromatous renal artery stenosis.[Clin Exp Nephrol. 2013]Review Diagnosis and therapy of atheromatous renal artery stenosis.Tanemoto M. Clin Exp Nephrol. 2013 Dec; 17(6):765-70. Epub 2013 Mar 26.
- Review Treatment of hypertension in patients with atherosclerotic renal artery stenosis, updated.[Postgrad Med. 2014]Review Treatment of hypertension in patients with atherosclerotic renal artery stenosis, updated.Chrysant SG. Postgrad Med. 2014 Nov; 126(7):59-67.
- [The changing etiology and therapeutic situation of atherosclerotic renal artery stenosis].[Zhonghua Yi Xue Za Zhi. 2005][The changing etiology and therapeutic situation of atherosclerotic renal artery stenosis].Wang F, Wang M, Liu YC, Wang HY. Zhonghua Yi Xue Za Zhi. 2005 Oct 19; 85(39):2762-6.
- Management of Atherosclerotic Renal Artery Stenosis - Comparative Effectiveness ...Management of Atherosclerotic Renal Artery Stenosis - Comparative Effectiveness Review Summary Guides for Clinicians
- Chmp4c charged multivesicular body protein 4C [Mus musculus]Chmp4c charged multivesicular body protein 4C [Mus musculus]Gene ID:66371Gene
Your browsing activity is empty.
Activity recording is turned off.
See more...