Testing for C. difficile
Patients with diarrhea and risk factors for CDI should undergo testing for C. difficile ().
The diagnosis of C. difficile infection (CDI) is based on the combination of both clinical findings (usually diarrhea), as well as laboratory or histopathological findings () for definition of CDI. Clinical severity can range from mild diarrhea to severe, fulminant colitis with paralytic ileus and toxic megacolon. Patients can also have asymptomatic carriage or colonization of Clostridioides difficile.
The following signs and symptoms suggest patients who exhibit these features should be tested for the disease. The most common symptom of CDI is diarrhea, defined as 3 or more loose or unformed stool in less than 24 hours, without an alternative cause (eg, laxative use, oral contrast, tube feed initiation). The stool may contain occult blood, but melena and hematochezia are atypical. Fever and abdominal pain are present in about 50% of patients, and can be markers for increasing disease severity. Leukocytosis (WBC >15,000 cells/mm3) occurs frequently and may actually precede diarrhea or other clinical symptoms.
The presence of pseudomembranes on lower endoscopy is essentially pathognomonic for CDI, and occurs in 50% of cases. Endoscopy is not needed for diagnostics, however, as stool studies are readily available and active CDI renders a patient at increased risk for endoscopic complications including perforation.
Less common signs and symptoms of CDI include arthralgias and reactive arthritis, as well as severe protein-wasting diarrhea with resultant hypoalbuminemia, edema and ascites.
Laboratory Testing Algorithms
Two- or three-stage testing algorithms are preferable to single-step methods.
The optimal rapid laboratory testing algorithm for presence of toxigenic C. difficile in stool has not been established, but there is evidence that two- or three-stage testing algorithms are preferable to single-step methods due to improved specificity.28
For UMHS testing algorithms see and .
When possible, testing should be limited to diarrheal stools unless the suspicion for CDI is high and an ileus is present. In select patients (immunocompromised, ileus, or on empiric therapy) the sensitivity of other rapid tests can be low and ID consultation and PCR-based testing should be considered (Appendix A).
The gold standard for organism detection is cytotoxigenic culture and the corresponding gold standard for toxin detection is the cell cytotoxicity assay.29 Both methods require considerable time and expense and are now rarely performed by clinical laboratories.
An overview of symptoms consistent with CDI is provided in . To avoid false-positive results (eg, positive C. difficile testing in the setting of colonization), only diarrheal stools (those that take the shape of the container) should be submitted for testing. Laxatives, tube feed initiation, and oral contrast can lead to loose or liquid stools prompting testing for C. difficile. C. difficile testing when there is an alternative cause of diarrhea may lead to identification of C. difficile colonization rather than true infection, and treatment of colonization is not recommended as it is not helpful and may even increase shedding of spores.
An exception to this is the case of patients with suspected CDI and ileus, in which case stool of any consistency can be considered for testing. If a patient with ileus and suspected CDI is unable to produce stool, a rectal swab for tcdB PCR can be sent for after consultation with ID. If a patient has an ileostomy with higher then baseline output (without an alternative explanation) then a stool specimen can be sent for CDI testing. In patients where there is concern for CDI involving the rectal stump, a rectal swab for direct tcdB PCR may be sent after consultation with ID. (For PCR testing at UMHS, after electronically placing an order for a C. difficile test, phone the lab to request PCR only from the swab. See Appendix A for available diagnostic tests for toxigenic C. difficile).
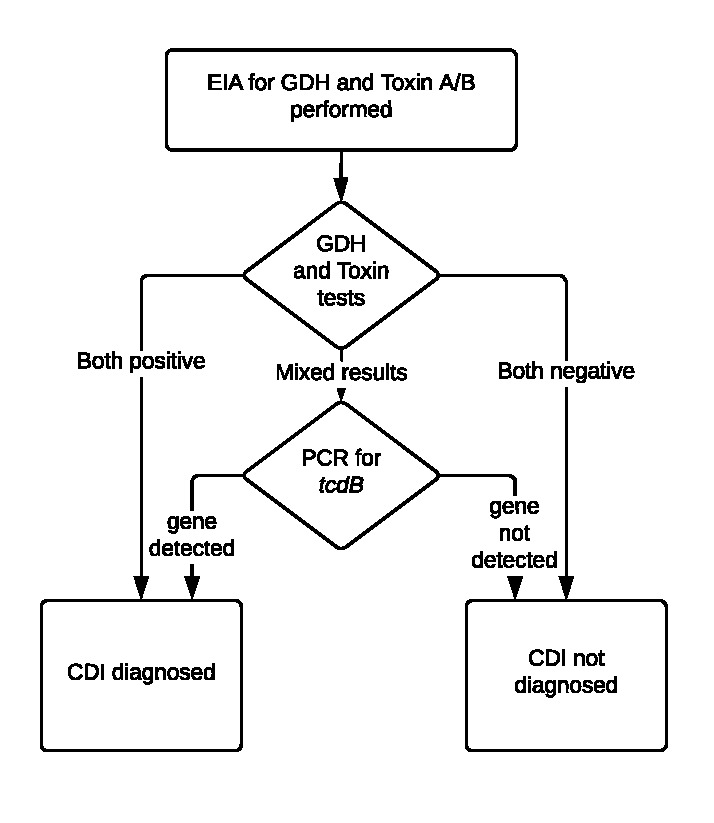
The recommended UMHS testing algorithm consists of two initial EIA tests (GDH and Toxins A/B), with reflex to a PCR test for tcdB gene for discordant results (). Data and recent guidelines support the use of multi-step over single-step testing with EIA for toxigenic C. difficile due to improved test characteristics, though single-step testing via PCR also performed well.28–32 This algorithm has been validated by our clinical laboratory and has a negative predictive value of 99%.33
There are circumstances when false-negative results can occur with EIA testing alone. Immunocompromised patients with symptoms suggestive of CDI (colitis on imaging, ileus with minimal stool production, and/or WBC >15,000 cells/µL with diarrhea) and patients receiving empiric therapy at the time of diagnosis are at risk for a false-negative EIA test.34 In these patients, if PCR testing was not performed, an ID consult and direct PCR for tcdB on stool or via rectal swab should be considered (at UMHS, ordered separately by phone). Finally, single-step PCR testing (not part of the UMHS algorithm) occurs as part of the new BioFire test panel for gastrointestinal pathogens (FilmArray, BioFire Diagnostics Inc., Salt Lake City, UT). This test should not be used if CDI is suspected, and providers should follow the recommendations in and order multi-step testing as indicated. If C. difficile is detected as part of the Biofire panel and the patient’s symptoms are compatible with CDI, then a separate order for multi-step testing is unnecessary and providers should refer to our treatment algorithm () and begin therapy as indicated.29
Imaging.
In patients with abdominal distention and suspicion for CDI, radiologic evaluation may serve as a useful diagnostic adjunct. This is especially true if there is a concern for CDI-induced ileus or toxic megacolon. Plain film abdominal x-rays may show dilated colon or ileus pattern. If free air is present on x-ray imaging, emergent surgical consult is warranted.35,36
In patients who present with abdominal pain, significant abdominal distention, or other signs of fulminant CDI, computed tomography (CT) of the abdomen and pelvis may be considered for further evaluation. Findings on CT may include colonic wall thickening, ascites, megacolon (distension of the colon of >6 cm in transverse width), ileus or perforation.37 Overall CT sensitivity for diagnosis of C. difficile colitis is 52–85%, with specificity of 48–93%.38
The use of enteral, intravenous and rectal contrast is preferred by UMHS Acute Care Surgery group, unless otherwise contraindicated. Some institutions advocate a more rigid adherence to CT scan diagnostic criteria for C. difficile colitis of colon wall thickening of greater than 4 mm combined with any one or more findings of pericolonic stranding, colon wall nodularity, the “accordion” sign (alternating edematous haustral folds separated by transverse mucosal ridges filled with oral contrast material, simulating the appearance of an accordion39), or otherwise unexplained ascites, with a reported sensitivity of 70% and specificity of 93%38 ().
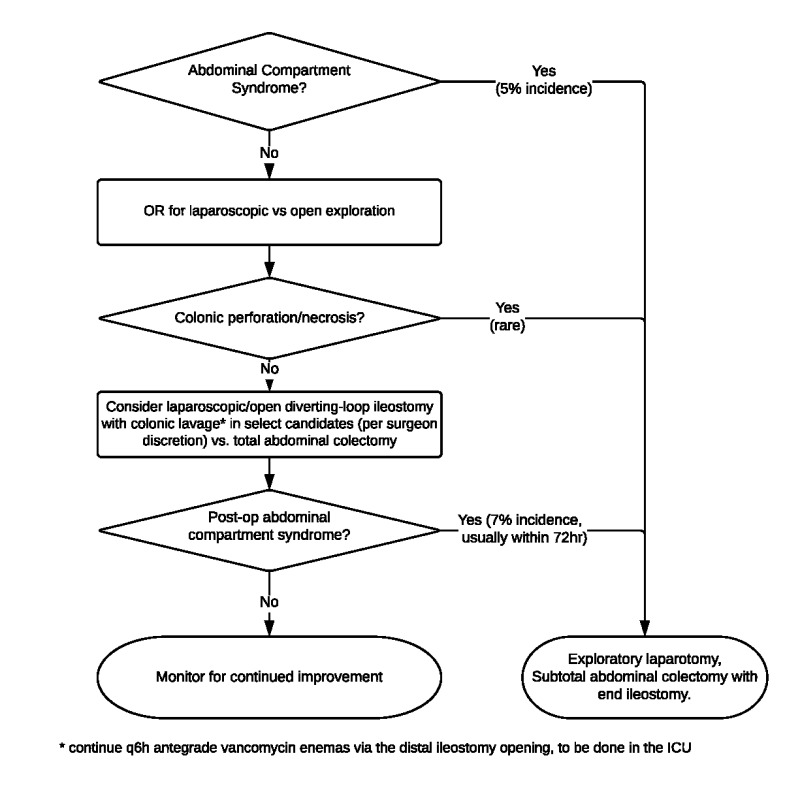
Patients who have CT findings concerning for severe or fulminant CDI, or who are critically ill with documented severe CDI warrant early surgical consultation. Specific findings have not been shown to reliably predict the need for surgical intervention.38,40 However, early involvement of a general surgeon may initiate discussions of treatment options, including consideration for diverting loop ileostomy for antegrade colonic irrigation. (Refer to section on surgical management, ).
Endoscopy.
Colonoscopy may be useful in patients with persistent diarrhea despite negative C. difficile toxin or with toxin-positive CDI refractory to antibiotics. In patients with positive stool testing for CDI, a colonoscopy is not necessary for diagnosis given that pseudomembranes are present only in 50% of patients with toxin-positive CDI.41 Additional indications to perform a colonoscopy in toxin-positive CDI patients include the assessment of CDI severity and the management of severe colonic distension associated with ileus. It is worth noting that a negative flexible sigmoidoscopy does not rule out CDI as sparing of the rectosigmoid colon is common in CDI patients with pseudomembranes on colonoscopy.42
Colonoscopy is contraindicated, especially for diagnostic purposes, in patients with hemodynamic instability or with significant risk for bowel perforation (eg, fulminant colitis, recent bowel surgeries, bowel obstruction).
Differential Diagnosis of Diarrhea.
C. difficile-toxin negative patients with persistent diarrhea should be evaluated further with colonoscopy with random biopsies and esophagogastroduodenoscopy (EGD), with duodenal biopsies for inflammatory and non-inflammatory causes of persistent diarrhea. Inflammatory diarrhea includes inflammatory bowel disease (ulcerative colitis and Crohn’s disease), celiac disease, microscopic colitis (collagenous and lymphocytic colitis), CMV (in immunocompromised hosts), and routine enteric pathogens when patients have exposure history or risk factors. Non-inflammatory causes include, dietary intolerance (lactose, fructose, or rapidly fermentable, short-chain carbohydrates [“FODMAP”43]) or small intestinal bacterial overgrowth in patients with significant abdominal bloating. Functional etiologies (irritable bowel syndrome) should be considered when workup is negative for inflammatory and non-inflammatory diarrhea.