View in own window
|
Updates, Authorship, and Related Guidelines
|
|
Developer and funding source
|
New York State Department of Health AIDS Institute (NYSDOH AI)
|
|
Intended users
|
Clinicians in New York State who provide ambulatory, inpatient, and emergency medical care for adults ≥18 years old who present with signs or symptoms of acute HIV infection or report an exposure within the past 4 weeks
|
|
Development
|
See Supplement: Guideline Development and Recommendation Ratings
|
|
Updates
|
|
July 19, 2021
|
Recommendations on diagnosis of acute HIV infection have been updated in the Presentation and Diagnosis section:
Clinicians can presume the diagnosis of acute HIV when high levels (>10,000 copies/mL) of HIV RNA are detected in plasma with sensitive NAT, and the result of the HIV screening or type-differentiation test is negative or indeterminate. (A2) Clinicians should seek expert consultation when an ambiguous HIV result is obtained for an individual taking PrEP because the diagnosis of acute HIV can be particularly challenging in patients taking PrEP. (A3) When a low-level quantitative HIV RNA viral load result (<10,000 copies/mL) is obtained in the absence of serologic evidence of HIV infection, the clinician should repeat HIV RNA testing and perform an Ag/Ab combination immunoassay to exclude a false-positive result. (A2)
Recommendations on HIV transmission and resistance have been updated in the Management, Including While on PEP or PrEP section:
Clinicians should inform patients about the increased risk of transmitting HIV during acute infection and for the 6 months following infection in patients who do not initiate ART. (A2) Patients taking PrEP: Because the risk of drug-resistant mutations is higher in patients who acquire HIV while taking PrEP, clinicians should consult with an experienced HIV care provider and recommend a fully active ART regimen. (A3)
|
|
Author and writing group conflict of interest disclosures
|
See Conflict of Interest statement*
|
|
Related NYSDOH AI guidelines
|
|
Purpose of This Guideline
Date of current publication: July 19, 2021
Lead author: Ethan Cowan, MD, MS
Writing group: Joseph P. McGowan, MD, FACP, FIDSA; Steven M. Fine, MD, PhD; Rona Vail, MD; Samuel T. Merrick, MD; Asa Radix, MD, MPH, PhD; Christopher J. Hoffmann, MD, MPH; Charles J. Gonzalez, MD
Committee:
Medical Care Criteria Committee
Date of original publication: August 24, 2018
This guideline on diagnosis and management of acute HIV infection was developed by the Medical Care Criteria Committee of New York State Department of Health AIDS Institute (NYSDOH AI) to guide clinicians in NYS who provide ambulatory, inpatient, and emergency medical care for adults ≥18 years old who present with signs or symptoms of acute HIV infection or report an exposure within the past 4 weeks.
This guideline provides evidence-based clinical recommendations for the diagnosis and treatment of acute HIV infection in adults, with the goals of ensuring that NYS clinicians are able to:
Recognize the risks for and signs and symptoms of acute HIV, include HIV infection in the differential diagnosis, and consider HIV testing in any person who presents with signs and symptoms suggestive of influenza (“flu”), mononucleosis (“mono”), or other viral syndromes, including suspected COVID-19.
Perform appropriate diagnostic and confirmatory testing when HIV infection is suspected and manage the treatment of acute HIV.
Meet the NYS requirements for reporting and partner notification.
Recommend or offer immediate initiation of antiretroviral therapy (ART) to improve the patient’s health and reduce the risk of HIV transmission; refer and confirm that patients can access optimal HIV care.
Initiate or refer the patient for prevention services.
View in own window
| TERMINOLOGY |
|---|
Acute HIV infection: Describes the period immediately after infection with HIV when an individual is viremic and has detectable p24 antigen or has HIV RNA without diagnostic HIV antibodies. In the medical literature, “primary HIV infection” may describe this same period. Recent infection: Generally used to describe the 6-month period after infection occurs. Early infection: May refer to acute or recent infection, after which infection is defined as chronic.
|
Early diagnosis for early treatment: Accumulating evidence supports a decision to begin HIV treatment at the time of diagnosis [Lundgren, et al. 2015]. Initiation of ART during acute infection may have several beneficial clinical outcomes, including improved preservation of immunologic function, significantly reduced time to viral suppression, and reduction of the viral reservoir, which could be important for cure strategies [Pires, et al. 2004; Streeck, et al. 2006; Koegl, et al. 2009; Hocqueloux, et al. 2010; Ananworanich, et al. 2012; Buzon, et al. 2012; Lafeuillade, et al. 2012; Margolick, et al. 2015; Phanuphak, et al. 2015; Le, et al. 2013; Saez-Cirion, et al. 2013; Pilcher, et al. 2017]. The risk of sexual transmission of HIV during acute or recent infection is significantly higher than during chronic infection [Pilcher, et al. 2004; Hollingsworth, et al. 2008; Pinkerton 2008; Hollingsworth, et al. 2015]; this difference likely correlates with high levels of viremia and is consistent with other routes of transmission [Bellan, et al. 2015]. The public health benefit of early ART initiation is well documented, with a significant reduction of HIV transmission among virally suppressed individuals. Further, in September 2017, the NYSDOH endorsed the consensus from the Prevention Access Campaign that undetectable = untransmittable (“U = U”), which indicates that individuals with a durable (≥6 months) undetectable viral load will not sexually transmit HIV [NYSDOH 2017; Prevention Access Campaign 2018].
Recognizing and diagnosing acute HIV infection is crucial to linking patients to care early and presents an important opportunity to reduce HIV transmission. Factors that may contribute to the increased risk for transmission during acute infection include:
Hyperinfectivity associated with both markedly high viral load levels (often much greater than 10 million viral copies/mm
3) and increased infectiousness of the virus [
Quinn, et al. 2000;
Ma, et al. 2009].
For many reasons, detecting acute HIV infection is an essential link in the chain of prevention. Evidence demonstrates that patients with a recent diagnosis of HIV are more likely to reduce risk behaviors if they are given counseling at the time of testing [Steward, et al. 2009; Fonner, et al. 2012] and are linked to primary HIV care [Metsch, et al. 2008]. In addition, for those who elect to initiate ART, their risk of transmission is significantly diminished [Cohen, et al. 2011; Cohen, et al. 2016].
View in own window
| Key Points |
|---|
HIV is highly transmissible during acute infection; rapid initiation of antiretroviral therapy (ART) reduces transmission, with significant public health benefits, and early viral suppression preserves immune function, with significant clinical benefits for the individual with HIV. Acute HIV often has nonspecific signs and symptoms and often goes unsuspected and undetected. This committee urges a high index of suspicion for acute infection and HIV testing for any individual who reports recent high-risk behavior or presents with signs or symptoms of influenza, mononucleosis, or other viral syndromes. When HIV infection is diagnosed, immediate linkage to care is essential; ART dramatically reduces HIV-related morbidity and mortality, and viral suppression prevents HIV transmission. The urgency of ART initiation is even greater if the newly diagnosed patient is pregnant, has acute HIV infection, is ≥50 years old, or has advanced disease. For these patients, every effort should be made to initiate ART immediately, ideally on the same day as diagnosis. All clinical care settings should be prepared, either on-site or with a confirmed referral, to support patients in initiating ART as rapidly as possible after diagnosis. When a diagnosis of acute HIV infection is made, clinicians should discuss the importance of notifying all recent contacts and refer patients to partner notification services, as mandated by New York State law. The NYSDOH can provide assistance if necessary.
|
Note on “experienced” and “expert” HIV care providers: Throughout this guideline, when reference is made to “experienced HIV care provider” or “expert HIV care provider,” those terms are referring to the following 2017 NYSDOH AI definitions:
Experienced HIV care provider: Practitioners who have been accorded HIV Experienced Provider status by the American Academy of HIV Medicine or have met the HIV Medicine Association’s definition of an experienced provider are eligible for designation as an HIV Experienced Provider in New York State. Nurse practitioners and licensed midwives who provide clinical care to individuals with HIV in collaboration with a physician may be considered HIV Experienced Providers as long as all other practice agreements are met (8 NYCRR 79-5:1; 10 NYCRR 85.36; 8 NYCRR 139-6900). Physician assistants who provide clinical care to individuals with HIV under the supervision of an HIV Specialist physician may also be considered HIV Experienced Providers (10 NYCRR 94.2)
Expert HIV care provider: A provider with extensive experience in the management of complex patients with HIV.
Presentation and Diagnosis
View in own window
| RECOMMENDATIONS |
|---|
|
New York State HIV Testing Requirements
According to New York State law, physicians must offer an HIV test to all patients aged 13 years and older (or younger with risk) if a previous test is not documented, even in the absence of symptoms consistent with acute HIV. Although written consent to HIV testing is no longer required in New York State, patients must be given the opportunity to decline, and verbal consent must be documented in the medical record.
Presentation
Clinicians should include acute HIV infection in the differential diagnosis for anyone (regardless of reported risk) who presents with signs or symptoms of influenza (“flu”), mononucleosis (“mono”), or other viral syndromes (A3), especially when the patient:
Presents with a rash. (A2) Requests HIV testing. (A3) Reports recent sexual or parenteral exposure to a person with or at risk of HIV infection. (A2) Presents with a newly diagnosed STI. (A2) Presents with aseptic meningitis. (A2) Is pregnant or breastfeeding. (A3) Is currently taking antiretroviral medications for PrEP or PEP. (A3)
Diagnostic HIV RNA testing should be considered for patients who present with compatible symptoms (see Box 1: Acute Retroviral Syndrome), particularly in the presence of an STI [ Patel, et al. 2006] or a recent sexual or parenteral exposure with a partner known to have HIV or with unknown HIV serostatus. (A2)
When Acute HIV Infection Is Suspected
Diagnosis
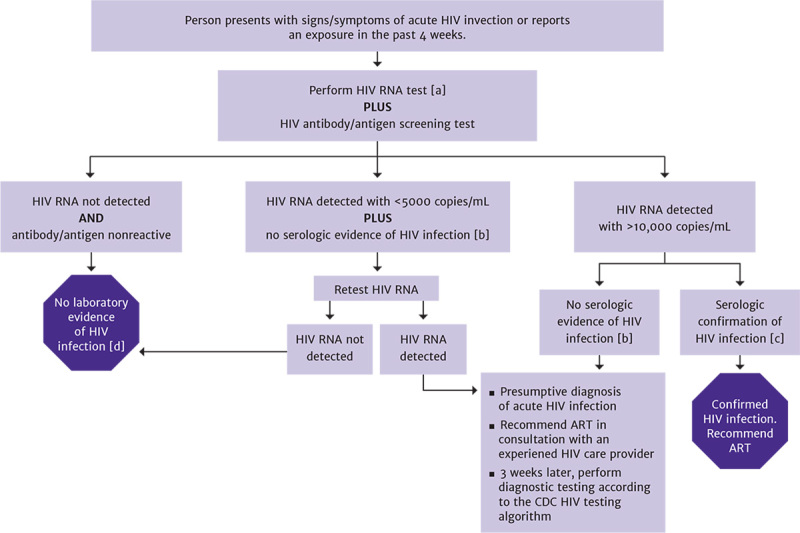
Clinicians can presume the diagnosis of acute HIV when high levels (>10,000 copies/mL) of HIV RNA are detected in plasma with sensitive NAT, and the result of the HIV screening or type-differentiation test is negative or indeterminate. (A2) When a low-level quantitative HIV RNA viral load result (<10,000 copies/mL) is obtained in the absence of serologic evidence of HIV infection, the clinician should repeat HIV RNA testing and perform an Ag/Ab combination immunoassay to exclude a false-positive result. (A2)
Clinicians should seek expert consultation when an ambiguous HIV result is obtained for an individual taking PrEP because the diagnosis of acute HIV can be particularly challenging in patients taking PrEP. (A3)
ART Initiation
If a diagnosis of acute infection is made based on HIV RNA testing, clinicians should recommend ART initiation without waiting for serologic confirmation. (A2) When a pregnant individual is diagnosed with acute infection by HIV RNA testing, the clinician should not wait for the result of a confirmatory test to initiate ART; initiation of ART is strongly recommended for pregnant patients. (A2)
Partner Notification
|
Abbreviations: Ab, antibody; Ag, antigen; ART, antiretroviral therapy; NAT, nucleic acid test; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.
The time from HIV infection to detection of the virus depends on the test that is used. Figure 1, below, illustrates the window of detection of HIV infection according to Ab, Ag/Ab combination, and HIV RNA tests.
Presentation
Patients acutely infected with HIV will often experience at least some symptoms of acute retroviral syndrome (ARS). Fever and influenza- or mononucleosis-like symptoms are common in acute HIV infection but are nonspecific. Rash, mucocutaneous ulcers, oropharyngeal candidiasis, and meningismus are more specific and should raise the index of suspicion (see below for a more extensive list of signs and symptoms). The mean time from exposure to onset of symptoms is generally 2 to 4 weeks, with a range of 5 to 29 days; however, some cases have presented with symptoms up to 3 months after exposure [Apoola, et al. 2002]. Theoretically, this time course may be prolonged in patients who become infected while on PEP or PrEP.
View in own window
| Box 1: Acute Retroviral Syndrome |
|---|
|
Signs and symptoms of ARS with the expected frequency among symptomatic patients are listed below [a]. The most specific symptoms in this study were oral ulcers and weight loss; the best predictors were fever and rash. The index of suspicion should be high when these symptoms are present.
Fever (80%) Tired or fatigued (78%) Malaise (68%) Arthralgias (joint pain) (54%) Headache (54%) Loss of appetite (54%) Rash (51%) Night sweats (51%) Myalgias (pain in muscles) (49%) Nausea (49%) Diarrhea (46%) Fever and rash (46%) Pharyngitis (sore throat) (44%) Oral ulcers (mouth sores) (37%) Stiff neck (34%) Weight loss (>5 lb; 2.5 kg) (32%) Confusion (25%) Photophobia (24%) Vomiting (12%) Infected gums (10%) Sores on anus (5%) Sores on genitals (2%)
|
- a
Data are from Hecht FM, Busch MP, Rawal B, et al. Use of laboratory tests and clinical symptoms for identification of primary HIV infection. AIDS 2002;16(8):1119-1129. [PMID: 12004270]
Diagnosis
Acute HIV infection is often not recognized in the primary care setting because the symptom profile is similar to that of influenza, mononucleosis, and other common illnesses. Furthermore, patients often do not recognize that they may have recently been exposed to HIV. Therefore, the clinician should have a high index of suspicion for acute HIV infection in a patient who may have recently engaged in behavior involving sexual or parenteral exposure to another individual’s blood or body fluids and who is presenting with a febrile, influenza-, or mononucleosis-like illness. Identifying acute HIV infection during pregnancy is particularly important because effective intervention can prevent mother-to-child transmission [Patterson, et al. 2007].
High levels of HIV RNA detected in plasma through sensitive NAT, combined with a negative or indeterminate HIV screening or type-differentiation test, support the presumptive diagnosis of acute HIV infection [Robb, et al. 2016; DHHS 2019].
When low-level viremia is reported by HIV RNA testing (<5,000 copies/mL) in the absence of serologic confirmation of HIV infection, HIV RNA testing should be repeated to exclude a false-positive result [Hecht, et al. 2002]. Repeat HIV RNA testing with a result that indicates the presence of low-level viremia may represent true HIV infection, warranting appropriate counseling regarding transmission risk and initiation of ART.
HIV RNA levels tend to be very high in acute infection; however, a low value may represent any point on the upward or downward slope of the viremia associated with acute infection or could simply represent chronic infection. HIV RNA can also be suppressed during acute infection in patients who are taking PrEP. Plasma HIV RNA levels during acute infection do not appear significantly different in patients who are and are not symptomatic [Patterson, et al. 2007]. Viremia occurs approximately 1 to 2 weeks before the detection of a specific immune response. Patients diagnosed with acute infection by HIV RNA testing should always receive follow-up diagnostic testing 3 weeks later to confirm infection (see the standard HIV laboratory testing algorithm). Figure 2, below, illustrates diagnostic testing for acute HIV infection.
View in own window
| Key Points |
|---|
The diagnosis of acute HIV infection requires a high degree of clinical awareness. The nonspecific signs and symptoms of acute HIV infection are often not recognized or attributed to another viral illness. Diagnostic HIV RNA testing should be considered for all patients who present with compatible symptoms (see signs and symptoms of ARS, above), particularly in the context of an STI [ Patel, et al. 2006] or a recent sexual or parenteral exposure with a partner known to have HIV or a partner whose HIV serostatus is not known. Individual laboratories have internal protocols for reporting HIV tests with preliminary results. The terms used when preliminary results cannot be classified include indeterminate, inconclusive, nondiagnostic, and pending validation. Clinicians can contact the appropriate laboratory authority to determine the significance of nondefinitive results and the recommended supplemental testing, particularly when acute HIV infection is suspected. Clinicians are advised to become familiar with the internal test-reporting policies of their institutions.
|
Management, Including While on PEP or PrEP
View in own window
| RECOMMENDATIONS |
|---|
|
Managing Acute HIV
Clinicians should recommend ART to all patients diagnosed with acute HIV infection. (A1) Clinicians should inform patients about the increased risk of transmitting HIV during acute infection and for the 6 months following infection in patients who do not initiate ART. (A2) As part of the initial management of patients diagnosed with acute HIV infection, clinicians should:
Consult with a care provider experienced in the treatment of acute HIV infection. (A3) Obtain HIV genotypic resistance testing for the protease (A2), reverse transcriptase (A2), and integrase (B2) genes at the time of diagnosis.
Patients taking PEP: When acute HIV infection is diagnosed in an individual receiving PEP, ART should be continued pending consultation with an experienced HIV care provider. (A3) Patients taking PrEP: Because the risk of drug-resistant mutations is higher in patients who acquire HIV while taking PrEP, clinicians should consult with an experienced HIV care provider and recommend a fully active ART regimen. (A3)
Initiating ART
When a patient agrees with the clinician’s recommendation to initiate ART during acute HIV infection:
|
Abbreviations: ART, antiretroviral therapy; PEP, post-exposure prophylaxis; PrEP, pre-exposure prophylaxis.
Patients are at greatest risk for transmitting HIV during periods of high viremia early in infection. Clinicians should counsel patients with acute HIV about the increased risk of transmission during the 6 months after infection. Partner notification [Golden, et al. 2004], counseling on safer sex, and screening for other sexually transmitted infections are all essential in the management of any new HIV diagnosis.
Consultation: When choosing an ART regimen for a patient with acute HIV infection, clinicians should consult a care provider experienced in treating acute HIV infection.
The risks of transmitted resistance should be considered when prescribing ART while awaiting HIV resistance results.
The risks of acquired mutations should be considered in those who acquire HIV while on PrEP.
Clinicians who do not have access to experienced HIV care providers should call the CEI Line at 866-637-2342.
Benefits and Risks of ART
This section is an excerpt from the NYSDOH AI guideline Rapid ART Initiation
ART is the use of pharmacologic agents that have specific inhibitory effects on HIV replication. These agents belong to distinct classes of drugs with different mechanisms of action.
A list of all commercially available antiretroviral (ARV) drugs that are approved by the U.S. Food and Drug Administration for the treatment of HIV/AIDS is available here.
Benefits of ART
ART has led to dramatic reductions in HIV-associated morbidity and mortality [CDC(a) 2022]. In resource-rich settings, life expectancy of patients with HIV infection with access to early ART is approaching that of the general population [Xia, et al. 2022; Siddiqi, et al. 2016]. A number of randomized clinical trials have demonstrated the benefits of ART in reducing HIV-related morbidity and mortality, irrespective of the degree of immune suppression at treatment initiation [Lundgren, et al. 2015; Severe, et al. 2010]. Thus, ART should be recommended to all individuals with HIV infection.
With proper selection of an initial regimen (see the NYSDOH AI guideline Selecting an Initial ART Regimen) and good patient adherence, durable virologic suppression (i.e., lifetime control of viral load) is achieved in virtually all patients with HIV. Virologic suppression almost invariably leads to immunologic recovery, followed by reductions in the incidence of opportunistic infections and malignancies.
The measurable goals of treatment include:
Viral suppression as measured by an HIV-1 RNA level below the limits of detection
Immune reconstitution as measured by an increase in or maintenance of CD4 cell count
Reduction in HIV-associated complications, including AIDS-related and non-AIDS-related conditions
ART also reduces morbidity and mortality from causes not related to HIV. In a randomized study comparing continuous ART with CD4-guided treatment interruption, a mortality benefit was observed in participants on continuous ART [El-Sadr, et al. 2006]. This benefit was attributed to a reduction in deaths from cardiovascular, renal, and hepatic causes. ART decreases the inflammatory milieu associated with ongoing HIV replication. It is postulated that ART-mediated reductions in proinflammatory cytokines lead to lower rates of clinical complications associated with the proinflammatory state [Hileman and Funderburg 2017].
Reduced HIV transmission: ART for people with HIV is now part of the established strategy aimed at reducing HIV transmission and is an essential component of prevention interventions along with risk-reduction counseling, safer-sex practices, avoidance of needle-sharing, and HIV pre-exposure and post-exposure prophylaxis (PrEP and PEP; see the NYSDOH AI guidelines PrEP to Prevent HIV and Promote Sexual Health and PEP to Prevent HIV Infection). Antiretroviral treatment as prevention is associated with greater reductions in HIV transmission than any preventative modality studied to date. In HPTN 052, a large randomized clinical trial of HIV-serodifferent couples, early treatment of the partner with HIV was associated with a 96% reduction in HIV transmission compared with a delayed treatment approach [Cohen, et al. 2011]. In long-term follow-up of study participants, linked transmissions between partners were found to occur only when the index partner was viremic [Cohen, et al. 2016]. In observational studies, including the Opposites Attract, PARTNER, and PARTNER2 studies, no phylogenetically linked HIV transmission was observed in serodifferent couples in which the index partner was virologically suppressed on ART [Rodger, et al. 2019; Bavinton, et al. 2018; Rodger, et al. 2016]. The evidence thus suggests that the risk of sexual transmission of HIV during virologic suppression is negligible. ART should be recommended to all patients with HIV infection to prevent transmission to sex partners and, by extrapolation, to needle-sharing partners. Despite its potent benefit in reducing HIV transmission, ART does not obviate the use of condoms or clean syringes. Those harm reduction measures, along with the use of HIV PrEP for partners who do not have HIV infection, will help reduce the incidence of other sexually transmitted infections and viral hepatitis and should be integrated into patient counseling at ART initiation.
Reduced perinatal HIV transmission: Studies have shown that the administration of ART during pregnancy or intrapartum significantly reduces the risk of perinatal HIV transmission [Cohen, et al. 2011; Guay, et al. 1999; Connor, et al. 1994], adding to the body of evidence that lower viral load reduces transmission risk.
Reduced complications: Accumulating evidence suggests that early initiation of ART or reduced cumulative time with detectable plasma viremia is associated with reductions in the likelihood of certain complications, such as cardiovascular disease, neurocognitive dysfunction, severe bacterial infections, and some non-HIV-related malignancies, and delayed initiation of ART is associated with long-term disparities in clinical outcomes [Lundgren, et al. 2023; O'Connor, et al. 2017; Ho, et al. 2012; Sigel, et al. 2012; Winston, et al. 2012; Ellis, et al. 2011; Garvey, et al. 2011; Silverberg, et al. 2011; Ho, et al. 2010; Lichtenstein, et al. 2010; Bruyand, et al. 2009; Guiguet, et al. 2009; Marin, et al. 2009; Tozzi, et al. 2007; El-Sadr, et al. 2006]. Cohort data also demonstrate that although older patients are more likely than younger patients to achieve virologic suppression, they are less likely to achieve an immunologic response, as measured by an increase of CD4 count by 100 cells/mm3, and that patients ≥55 years old may be at higher clinical risk even after starting ART [Sabin, et al. 2008]. The poor immunologic recovery seen in older patients is associated with higher morbidity and mortality, particularly cardiovascular events [van Lelyveld, et al. 2012]. In one study, men ≥50 years old with CD4 counts of 351 to 500 cells/mm3 who initiated ART were able to achieve similar immunologic responses as younger men who initiated at lower CD4 cell counts [Li, et al. 2011].
Risks of ART
Despite the excellent tolerability of contemporary ART regimens, adverse effects, long-term drug toxicities, and drug-drug interactions continue to pose some relative or limited risk, which necessitates patient counseling about the potential for ART-associated adverse events in the short and long term. These risks include tolerability issues, which may affect quality of life, and possible long-term toxicities—primarily a low relative risk of renal and cardiovascular disorders or decreased bone density of uncertain clinical significance [Hoy, et al. 2017; Monteiro, et al. 2014; Friis-Moller, et al. 2010]. Excess weight gain has been observed in patients receiving regimens containing integrase strand transfer inhibitors (e.g., dolutegravir and bictegravir) and/or tenofovir alafenamide but the clinical significance is unknown, and investigation is needed [Palella, et al. 2023; Verburgh, et al. 2022; Bourgi(a), et al. 2020; Bourgi(b), et al. 2020]. Renal and bone density issues are largely eliminated with newer formulations of ARV medications. Fatal drug reactions from ART are exceedingly rare.
Many ARV combinations are now available in single-pill, fixed-dose combination formulations. Thus, the pill burden associated with early ART regimens has been largely eliminated. Nevertheless, lifelong adherence to medications may constitute a challenge to some, particularly when treatment with a single daily tablet is not feasible.
Compared with early ARV combinations, current preferred ART regimens (see the NYSDOH AI guideline Selecting an Initial ART Regimen) are associated with higher rates of durable virologic suppression. Lack of virologic suppression in a patient on ART should prompt the clinician to evaluate patient adherence and provide intensive support to those reporting challenges in this domain. Failure to achieve and maintain virologic suppression may lead to the emergence of resistance-associated mutations (RAMs). A large cohort study demonstrated that virologic failure with contemporary ART regimens is associated with the infrequent emergence of RAMs [Scherrer, et al. 2016]. Nevertheless, RAMs can emerge with current first-line therapies. Resistance to ARV medications may compromise the potential for long-term virologic suppression, simple dosing schedules, and the tolerability of future treatment options.
ART initiation is associated with a risk of immune reconstitution inflammatory syndrome (IRIS). IRIS is a clinical syndrome characterized by new or worsening infectious and non-infectious complications observed after the initiation of ART (see the NYSDOH AI guideline Management of IRIS). The risk of IRIS increases when ART is begun at low CD4 cell counts (<100 cells/mm3) or with the presence of specific opportunistic infections [Manabe, et al. 2007]. Although the risk of IRIS is not a contraindication to initiating ART, clinicians and patients should be aware that the risk of developing IRIS is increased among individuals with low CD4 cell counts. Patients at increased risk should be informed of the potential for a paradoxical clinical worsening after ART initiation.
Risks of Untreated HIV
Results from the START trial [Lundgren, et al. 2015] and strong cohort data show that untreated HIV infection leads to increased morbidity and mortality from both HIV-related and non-HIV-related conditions, even at high CD4 cell counts. Together with the dramatic reduction in HIV transmission risk with effective treatment, these data support initiating ART regardless of CD4 cell count, including in patients diagnosed with acute HIV infection (see the NYSDOH AI guideline Diagnosis and Management of Acute HIV Infection). Patients in care who are documented long-term nonprogressors or elite controllers are a group that may warrant special consideration (see NYSDOH AI guideline Rapid ART Initiation > Special Considerations).
In START, a randomized clinical trial that compared initiating ART in treatment-naive patients with CD4 counts >500 cells/mm3 versus waiting for a decrease to ≤350 cells/mm3 before initiation, there was a 53% reduction in serious illness and death in the early ART group [Lundgren, et al. 2015]. Data from NA-ACCORD, a large observational cohort study, showed that both morbidity and mortality were improved by initiation of ART in patients with CD4 cell counts in the high or even normal range [Kitahata, et al. 2009]. A significantly decreased risk of death was observed in patients who initiated therapy at CD4 counts >500 cells/mm3 compared with those who deferred therapy until CD4 count was <500 cells/mm3, as well as in the cohort who initiated ART in the 350 to 500 cells/mm3 range compared with those who deferred until CD4 count was <350 cells/mm3 [Kitahata, et al. 2009]. Although other cohort studies demonstrated only a minimal survival advantage [Wright, et al. 2011] or no survival advantage among those starting ART at the highest CD4 cell counts, they did confirm the benefits of initiating ART at CD4 counts ≤500 cells/mm3 [Young, et al. 2012; Cain, et al. 2011; CASCADE Collaboration 2011]. Another study showed an approximately 33% reduction in the risk of death from end-stage liver disease, non-AIDS infections, and non-AIDS-defining cancers with each 100 cells/mm3 increase in CD4 count [Marin, et al. 2009]. A randomized study of early versus deferred therapy in patients with CD4 counts of 350 to 550 cells/mm3 showed no mortality benefit [Cohen, et al. 2011]; however, this study has significant limitations, most notably a relatively brief follow-up period.
Rationale for Rapid ART Initiation
This section is an excerpt from the NYSDOH AI guideline Rapid ART Initiation
View in own window
| RECOMMENDATIONS |
|---|
|
Rationale for Rapid ART Initiation
Clinicians should recommend antiretroviral therapy (ART) for all patients with a diagnosis of HIV infection. (A1) Clinicians should offer rapid initiation of ART—preferably on the same day (A1) or within 72 hours—to all individuals who are candidates for rapid ART initiation (see text) and who have:
A confirmed HIV diagnosis (A1), or A reactive HIV screening result pending results of a confirmatory HIV test (A2), or Acute HIV infection, i.e., are HIV antibody negative and HIV RNA positive (A2)
Clinicians should counsel patients with HIV-seronegative partners about the reduction of HIV transmission risk after effective ART is initiated and viral suppression is achieved and should strongly recommend ART for patients with HIV-seronegative partners. (A1) Clinicians should evaluate and prepare patients for ART initiation as soon as possible; completion of the following should not delay initiation:
Discuss benefits and risks of ART with the patient. (A3) Assess patient readiness. (A3) Identify and ameliorate factors that might interfere with successful adherence to treatment, including inadequate access to medication, inadequate supportive services, psychosocial factors, active substance use, or mental health disorders. (A2)
Clinicians should refer patients for supportive services as necessary to address modifiable barriers to adherence. An ongoing plan for coordination of care should be established. (A3) Clinicians should involve patients in the decision-making process regarding initiation of ART and which regimen is most likely to result in adherence. The patient should make the final decision of whether and when to initiate ART. (A3) If the patient understands the benefits of rapid initiation but declines ART, the clinician should revisit the topic of initiation as soon as possible. Clinicians should initiate ART in patients with advanced HIV (or AIDS) even if barriers to adherence are present; in these cases, referrals to specialized adherence programs should be made for intensified adherence support. (A2) After ART has been initiated, the clinician should monitor the patient’s response to therapy or consult with an experienced HIV care provider. (A2)
|
The NYSDOH AI HIV Clinical Guidelines Program and the U.S. Department of Health and Human Services (DHHS) recommend initiation of ART for all patients with a confirmed HIV diagnosis, regardless of their CD4 cell count or viral load, for the benefit of the individual with HIV (reduced morbidity and mortality) [Lundgren, et al. 2015; Zolopa, et al. 2009] and to reduce the risk of transmission to others [Cohen, et al. 2016]. Initiating ART during early HIV infection may improve immunologic recovery (CD4 T cell counts) and reduce the size of the HIV reservoir [Massanella, et al. 2021; Jain, et al. 2013]; evidence also shows that initiating ART at the time of diagnosis reduces treatment delays and improves retention in care and viral suppression at 12 months [Ford, et al. 2018].
View in own window
| KEY POINTS |
|---|
Rapid ART initiation, the standard of care in New York State, is efficacious, safe, and highly acceptable, with few patients declining the offer of immediate ART. Patients with active substance use, untreated mental health conditions, immigration issues, or unstable housing deserve the highest standard of HIV care, including the option of rapid ART initiation. Potential barriers to medication adherence and care continuity can be addressed with appropriate counseling and linkage to support services.
|
Reduced Treatment Delays and Loss to Follow-Up
Standard practice protocols for ART initiation have produced preventable delays, and the required wait for confirmatory HIV diagnostic and baseline laboratory test results (including resistance testing) along with required medical visits can unnecessarily delay the start of treatment by as long as 4 weeks. Problems in accessing insurance or waiting for activation of public benefits may also cause delays. It is estimated that in 2020, 82.4% of individuals diagnosed with HIV in the United States were linked to HIV medical care within 1 month of diagnosis [CDC(b) 2022]. Although not optimal, this reflects an increase since from 75.9% in 2016 [CDC(b) 2022], before the first reports of rapid ART initiation. Individuals with HIV who are not linked to care are at risk of having sustained viral loads and ongoing HIV transmission.
Rapid ART initiation may reduce delays and improve viral suppression rates in people with HIV. Rapid or same-day ART initiation, which is preferable, or initiation within 3 days of a newly positive HIV test is the strategy endorsed by the World Health Organization [WHO 2021] and is an essential component of the New York State Ending the Epidemic initiative. Mathematical modeling demonstrates that a test-and-treat strategy, with immediate initiation of ART and prevention approaches, could lead to elimination of new HIV infections [Granich, et al. 2009].
Benefits for the Patient With HIV
Shorter time to viral suppression: Several observational and clinical trials have demonstrated the individual-level benefits of rapid ART initiation [Ford, et al. 2018]. An early pilot of this approach in San Francisco, California, demonstrated that patients initiating ART within 1 or 2 days had a shorter time (median, 1.8 months) to viral suppression (HIV RNA ≤200 copies/mL) than those offered the standard of care (4.3 months) or than historical controls (7.2 months) [Pilcher, et al. 2017]. A longer-term follow-up of 225 patients at the same center found that, of patients who had access to rapid initiation, 95.8% had achieved viral suppression at least once and 92.1% had achieved it at the last recorded visit [Coffey, et al. 2019]. These individual-level benefits have been replicated in other U.S. and international studies that demonstrated improved viral suppression with shortened time to ART initiation [Mateo-Urdiales, et al. 2019; Mohammed, et al. 2019; Colasanti, et al. 2018; Koenig, et al. 2017; Rosen(b), et al. 2016]. After implementing rapid ART initiation at a hospital clinic in Atlanta, Georgia, time to viral suppression fell from 77 days, before the intervention, to 57 days [Lundgren, et al. 2015], and average time to ART initiation decreased from 21 to 7 days; both findings were statistically significant [Colasanti, et al. 2018]. After rollout of a city-wide rapid ART initiation program for people diagnosed with HIV in San Francisco, median time from first care visit to ART initiation decreased from 28 days to 1 day (by 96%) and median time from diagnosis to viral suppression decreased from 145 days to 76 days (by 46%) from 2013 to 2017 [Bacon, et al. 2021].
Increased retention in care: Rapid ART initiation leads to improved retention in care [Koenig, et al. 2017; Amanyire, et al. 2016; Rosen(b), et al. 2016]. In the RapIT trial in South Africa, patients newly diagnosed with HIV were randomized to rapid ART initiation or standard of care [Rosen(a), et al. 2016]. The participants in the rapid initiation arm had higher rates of ART initiation at 90 days (97% vs. 72%) and higher rates of retention in care and viral suppression (HIV RNA ≤400 copies/mL) at 10 months (relative risk, 1.26 [1.05-1.50]). The average cost per patient to achieve viral suppression was lower in the intervention arm, demonstrating that this strategy of care may also be cost-effective [Long, et al. 2017]. Studies conducted in China, the United States, and South Africa support the cost-effectiveness of rapid ART initiation [Benson, et al. 2020; Ford, et al. 2018; Wu, et al. 2015; Zulliger, et al. 2014]. Rapid ART initiation is efficacious, safe, and highly acceptable, with few patients declining the offer of immediate ART [Coffey, et al. 2019; Pilcher, et al. 2017].
Reduced HIV transmission: Modeling evidence suggests that rapid ART initiation may significantly reduce HIV transmission in the community, although this has been directly modeled only in the context of South Africa [Granich, et al. 2009]. In the United States, linkage to and retention in HIV care are significant gaps in the HIV care continuum, with an estimated 74.1% of individuals with HIV receiving any HIV care and 50.6% being retained in care during 2020 [CDC(b) 2022]. Models have translated these gaps in care to their effect on HIV transmission in the United States, demonstrating that between 43% and 49% of new HIV transmissions are attributable to individuals who have been diagnosed with HIV but are not receiving ART and have not been retained in care [Li, et al. 2019; Skarbinski, et al. 2015]. Because it is designed to help close this care gap, rapid ART initiation greatly reduces new HIV infections, hastening the achievement of HIV incidence reduction goals in New York State.
Rapid ART Initiation Is Safe
Preexisting resistance to currently recommended regimens for rapid initiation is rare. In the San Francisco study discussed previously [Pilcher, et al. 2017], 89.7% of patients used integrase strand transfer inhibitor (INSTI)-containing regimens and 12.8% used protease inhibitor-containing regimens. The predominant INSTI-based regimen was dolutegravir plus emtricitabine/tenofovir disoproxil fumarate. The clinic did not have any cases of major resistance mutations to the prescribed ART regimen, and no regimen switches were made because of resistance. Two patients had their regimens changed because of rash, and in 10 cases, the regimen was simplified to a single-tablet regimen. Obtaining and following up on baseline laboratory testing is important, because some medical conditions, such as renal insufficiency, may require a change to a patient’s ART regimen.
Of 149 patients initiating ART through a program in New York City, only 1 required a regimen change because of subsequently detected resistance [Pathela, et al. 2021].
Rapid ART initiation is safe. Most designated regimens for rapid ART initiation are the same regimens that are recommended for initial treatment in the existing NYSDOH, International Antiviral Society-USA, and DHHS guidelines. These regimens are well tolerated and effective, and the likelihood of drug resistance is low based on the current prevalence of drug resistance [NYCDHMH 2021].
View in own window
| Resources |
|---|
|
To identify or consult with an experienced HIV care provider in New York State, see the following:
|
Protocol for Rapid ART Initiation
This section is an excerpt from the NYSDOH AI guideline Rapid ART Initiation
View in own window
| RECOMMENDATIONS |
|---|
|
Protocol for Rapid ART Initiation
To determine whether a patient is a candidate for rapid ART initiation, the clinician should confirm that the individual has (A1):
A new reactive point-of-care HIV test result, a confirmed HIV diagnosis, suspected acute HIV infection, or known HIV infection, and No prior ART (i.e., treatment naive, excluding PrEP and PEP) or limited prior use of antiretroviral medications, and No medical conditions or specific opportunistic infections that require deferral of ART initiation, including suspected cryptococcal or TB meningitis and CMV retinitis
Clinicians should perform baseline laboratory testing listed in Box 2: Baseline Laboratory Testing Checklist for all patients who are initiating ART immediately; ART can be started while awaiting laboratory test results. (A3)
|
View in own window
| SELECTED GOOD PRACTICE REMINDERS |
|---|
|
Protocol for Rapid ART Initiation
Ensure that patients with a reactive HIV antibody screening test that is pending confirmation understand the benefits of rapid ART initiation, as well as the following:
Reactive screening test results are not formally diagnostic, because false-positive results are still possible. A confirmatory (diagnostic) HIV test will be performed. ART will be discontinued if the confirmatory test result is negative and continued if it is positive. The benefit of starting ART early, after a presumptive positive screening test, outweighs the negligible risk of taking ART for a few days and then stopping it if confirmed HIV negative.
Provide the result of the confirmatory HIV test as soon as it is available; discontinue ART if the result is negative and reinforce adherence and next steps if it is positive. If a patient declines rapid ART initiation, discuss options for deferral of ART initiation, link the patient with HIV primary care, and outline next steps.
|
Reactive HIV Screening Test Result
When the result of a patient’s initial HIV point-of-care screening test is reactive, established practice is to obtain a blood specimen for diagnostic HIV testing because of the possibility of false-positive screening results. This is particularly important for individuals who are not at high risk of acquiring HIV. However, supplemental testing results may not be available for several days, introducing the risk that a patient will not return. The goal of the rapid ART initiation protocol is to assess whether a patient with a reactive HIV screening test result (or a confirmed HIV diagnosis) is also a candidate for same-day initiation of ART. If so, then the rapid ART initiation protocol is to provide counseling on HIV transmission and the benefits of ART, initiate ART that day or within 3 days, and link the patient expeditiously to HIV primary care. Thus, the protocol recommends immediate initiation of ART while awaiting confirmatory HIV test results.
Patients who are candidates for rapid ART initiation:
Have a new reactive point-of-care HIV test result, a new HIV diagnosis (confirmed using the standard
HIV laboratory testing algorithm), suspected acute HIV infection (HIV antibody negative and HIV RNA positive), or known HIV,
andAre treatment naive or have limited prior use of antiretroviral medications (e.g., a patient who stopped first-line therapy for reasons other than regimen failure), excluding PEP or PrEP, as long as concern for acquired drug resistance is low (requires a case-by-case determination), and
Have no medical conditions or opportunistic infections that require deferral of ART initiation, including suspected cryptococcal or TB meningitis or CMV retinitis
Patients with a new reactive HIV test result can be retested using a second point-of-care test from a manufacturer different from that of the first test to further minimize the possibility of a false-positive result. It is not necessary to retest with a second point-of-care test before providing ART, but given the possibility of a false-positive screening result, a laboratory-based confirmatory HIV test should always be performed to establish a diagnosis of HIV. If the confirmatory HIV test result is negative, ART can be discontinued.
Counseling
A reactive HIV screening result should prompt a care provider to counsel the patient about the benefits and risks of ART and about HIV transmission risk, including the consensus that undetectable equals untransmittable (U=U). When patients initiate ART on the same day as their reactive HIV test result, the priorities for patient education and counseling include:
Confirming the diagnosis of HIV
Managing disclosure, if indicated
Adhering to the ART regimen
Ensuring the patient knows how to reach the care team to address any potential adverse effects of medications or other concerns
Following through with clinic visits
Assessing health literacy (see resources below)
Navigating acquisition of and paying for medications required for lifelong therapy, including pharmacy selection, insurance requirements and restrictions, copays, and prescription refills
Identifying and addressing psychosocial issues that may pose barriers to treatment
Referring for substance use and behavioral health counseling if indicated
Referring for housing assistance if indicated
View in own window
| RESOURCES: HEALTH LITERACY |
|---|
National Library of Medicine:
Agency for Healthcare Research and Quality:
|
Medical and Psychosocial Assessment
Medical assessment of a patient with a new reactive HIV test result should include history or signs or symptoms of opportunistic infection(s). ART should be delayed and appropriate medical management initiated if TB meningitis or cryptococcal meningitis are suspected (see below) [WHO 2021], if cytomegalovirus retinitis is suspected, or if the patient has any evidence of advanced HIV disease on clinical exam.
To identify the potential for preexisting drug-resistant virus, the initial assessment should also include the patient’s history of PrEP and PEP use and previous ART use for people who are re-engaging in care [Ford, et al. 2018]. See Box 1, below.
View in own window
| Box 1: Medical History Checklist |
|---|
|
When taking a medical history before rapid antiretroviral therapy (ART) initiation, ask about:
Date and result of last HIV test Serostatus of sex partners and their ART regimens if known Previous use of antiretroviral medications, including as pre- or post-exposure prophylaxis, with dates of use Comorbidities, including a history of renal or liver disease, particularly hepatitis B virus infection Prescribed and over-the-counter medications Drug allergies Substance use Psychiatric history, particularly depressive or psychotic symptoms or any history of suicidality Possible pregnancy and childbearing plans in individuals of childbearing potential
|
Deferral of ART initiation: If the patient understands the benefits of rapid initiation but declines ART, then initiation should be revisited as soon as possible. In some circumstances, such as in the rare case of suspected cryptococcal or TB meningitis, rapid ART is not recommended (see NYSDOH AI guideline Rapid ART Initiation > Special Considerations > Patients With Acute Opportunistic Infections). Patients who present with symptoms suggestive of CMV retinitis should be referred to an ophthalmologist for assessment and treatment. Patients who present with signs and symptoms suggestive of pulmonary or intracranial and ophthalmologic infections should receive further assessment before initiating ART on the same day as a reactive HIV screening test result.
ART initiation should be delayed in any person presenting with signs or symptoms suggestive of meningitis, including headache, nausea or vomiting, light sensitivity, and changes in mental status. Treatment of TB meningitis was investigated in a clinical trial in Vietnam in which immediate initiation of ART was compared with ART initiated 2 months after TB treatment [Torok, et al. 2011]. There were significantly more grade 4 adverse effects in individuals who initiated ART immediately than in those who delayed. Among patients with cryptococcal meningitis, early initiation of ART has been associated with adverse outcomes, including death [Boulware, et al. 2014]; therefore, it is recommended that ART be deferred until after the induction phase of treatment for cryptococcal meningitis has been completed (see U.S. Department of Health and Human Services Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents with HIV).
Cotreatment of HIV and pulmonary TB: It is clear that cotreatment of HIV and pulmonary TB improves survival. In the SAPIT trial in South Africa, there was a 56% relative reduction in mortality when ART was initiated within 4 weeks of TB treatment initiation, compared with when it was started after TB treatment was completed (hazard ratio, 0.44; 95% confidence interval, 0.25-0.79; P=.003), although symptoms of immune reconstitution inflammatory syndrome (IRIS) were greater in patients who started ART earlier [Abdool Karim, et al. 2010]. However, it is unclear whether ART initiation prior to initiation of pulmonary TB treatment is the best course of action. Care providers should weigh the benefits of rapid ART initiation against the potential drawbacks of pill burden, drug-drug interactions, and the risk of IRIS.
Baseline Laboratory and Resistance Testing
All patients with a reactive HIV test result should undergo the baseline laboratory testing listed in Box 2, below. For discussion of baseline testing, see the NYSDOH AI guideline Selecting an Initial ART Regimen > ART-Initiation Laboratory Testing. It is not necessary to wait for these test results before initiating ART.
View in own window
| Box 2: Baseline Laboratory Testing Checklist |
|---|
HIV-1/2 antigen/antibody immunoassay HIV quantitative viral load test Baseline HIV genotypic resistance profile Baseline CD4 cell count Testing for hepatitis A, B, and C viruses Comprehensive metabolic panel (creatinine clearance, hepatic profile) Pregnancy test for individuals of childbearing potential Urinalysis
|
All Recommendations
View in own window
| RECOMMENDATIONS |
|---|
|
New York State HIV Testing Requirements
According to New York State law, physicians must offer an HIV test to all patients aged 13 years and older (or younger with risk) if a previous test is not documented, even in the absence of symptoms consistent with acute HIV. Although written consent to HIV testing is no longer required in New York State, patients must be given the opportunity to decline, and verbal consent must be documented in the medical record.
Presentation
Clinicians should include acute HIV infection in the differential diagnosis for anyone (regardless of reported risk) who presents with signs or symptoms of influenza (“flu”), mononucleosis (“mono”), or other viral syndromes (A3), especially when the patient:
Presents with a rash. (A2) Requests HIV testing. (A3) Reports recent sexual or parenteral exposure to a person with or at risk of HIV infection. (A2) Presents with a newly diagnosed STI. (A2) Presents with aseptic meningitis. (A2) Is pregnant or breastfeeding. (A3) Is currently taking antiretroviral medications for PrEP or PEP. (A3)
Diagnostic HIV RNA testing should be considered for patients who present with compatible symptoms (see Box 1: Acute Retroviral Syndrome), particularly in the presence of an STI [ Patel, et al. 2006] or a recent sexual or parenteral exposure with a partner known to have HIV or with unknown HIV serostatus. (A2)
When Acute HIV Infection Is Suspected
Diagnosis
Clinicians can presume the diagnosis of acute HIV when high levels (>10,000 copies/mL) of HIV RNA are detected in plasma with sensitive NAT, and the result of the HIV screening or type-differentiation test is negative or indeterminate. (A2) When a low-level quantitative HIV RNA viral load result (<10,000 copies/mL) is obtained in the absence of serologic evidence of HIV infection, the clinician should repeat HIV RNA testing and perform an Ag/Ab combination immunoassay to exclude a false-positive result. (A2)
Clinicians should seek expert consultation when an ambiguous HIV result is obtained for an individual taking PrEP because the diagnosis of acute HIV can be particularly challenging in patients taking PrEP. (A3)
ART Initiation
If a diagnosis of acute infection is made based on HIV RNA testing, clinicians should recommend ART initiation without waiting for serologic confirmation. (A2) When a pregnant individual is diagnosed with acute infection by HIV RNA testing, the clinician should not wait for the result of a confirmatory test to initiate ART; initiation of ART is strongly recommended for pregnant patients. (A2)
Partner Notification
Managing Acute HIV
Clinicians should recommend ART to all patients diagnosed with acute HIV infection. (A1) Clinicians should inform patients about the increased risk of transmitting HIV during acute infection and for the 6 months following infection in patients who do not initiate ART. (A2) As part of the initial management of patients diagnosed with acute HIV infection, clinicians should:
Consult with a care provider experienced in the treatment of acute HIV infection. (A3) Obtain HIV genotypic resistance testing for the protease (A2), reverse transcriptase (A2), and integrase (B2) genes at the time of diagnosis.
Patients taking PEP: When acute HIV infection is diagnosed in an individual receiving PEP, ART should be continued pending consultation with an experienced HIV care provider. (A3) Patients taking PrEP: Because the risk of drug-resistant mutations is higher in patients who acquire HIV while taking PrEP, clinicians should consult with an experienced HIV care provider and recommend a fully active ART regimen. (A3)
Initiating ART
When a patient agrees with the clinician’s recommendation to initiate ART during acute HIV infection:
Benefits and Risks of ART
Rationale for Rapid ART Initiation
Clinicians should recommend antiretroviral therapy (ART) for all patients with a diagnosis of HIV infection. (A1) Clinicians should offer rapid initiation of ART—preferably on the same day (A1) or within 72 hours—to all individuals who are candidates for rapid ART initiation (see text) and who have:
A confirmed HIV diagnosis (A1), or A reactive HIV screening result pending results of a confirmatory HIV test (A2), or Acute HIV infection, i.e., are HIV antibody negative and HIV RNA positive (A2)
Clinicians should counsel patients with HIV-seronegative partners about the reduction of HIV transmission risk after effective ART is initiated and viral suppression is achieved and should strongly recommend ART for patients with HIV-seronegative partners. (A1) Clinicians should evaluate and prepare patients for ART initiation as soon as possible; completion of the following should not delay initiation:
Discuss benefits and risks of ART with the patient. (A3) Assess patient readiness. (A3) Identify and ameliorate factors that might interfere with successful adherence to treatment, including inadequate access to medication, inadequate supportive services, psychosocial factors, active substance use, or mental health disorders. (A2)
Clinicians should refer patients for supportive services as necessary to address modifiable barriers to adherence. An ongoing plan for coordination of care should be established. (A3) Clinicians should involve patients in the decision-making process regarding initiation of ART and which regimen is most likely to result in adherence. The patient should make the final decision of whether and when to initiate ART. (A3) If the patient understands the benefits of rapid initiation but declines ART, the clinician should revisit the topic of initiation as soon as possible. Clinicians should initiate ART in patients with advanced HIV (or AIDS) even if barriers to adherence are present; in these cases, referrals to specialized adherence programs should be made for intensified adherence support. (A2) After ART has been initiated, the clinician should monitor the patient’s response to therapy or consult with an experienced HIV care provider. (A2)
Protocol for Rapid ART Initiation
To determine whether a patient is a candidate for rapid ART initiation, the clinician should confirm that the individual has (A1):
A new reactive point-of-care HIV test result, a confirmed HIV diagnosis, suspected acute HIV infection, or known HIV infection, and No prior ART (i.e., treatment naive, excluding PrEP and PEP) or limited prior use of antiretroviral medications, and No medical conditions or specific opportunistic infections that require deferral of ART initiation, including suspected cryptococcal or TB meningitis and CMV retinitis
Clinicians should perform baseline laboratory testing listed in Box 2: Baseline Laboratory Testing Checklist for all patients who are initiating ART immediately; ART can be started while awaiting laboratory test results. (A3)
|
References
Amanyire G., Semitala F. C., Namusobya J., et al. Effects of a multicomponent intervention to streamline initiation of antiretroviral therapy in Africa: a stepped-wedge cluster-randomised trial.
Lancet HIV. 2016;3(11):e539–e548. [
PMC free article: PMC5408866] [
PubMed: 27658873]
Ananworanich J., Schuetz A., Vandergeeten C., et al. Impact of multi-targeted antiretroviral treatment on gut T cell depletion and HIV reservoir seeding during acute HIV infection.
PLoS One. 2012;7(3):e33948. [
PMC free article: PMC3316511] [
PubMed: 22479485]
Apoola A., Ahmad S., Radcliffe K. Primary HIV infection.
Int J STD AIDS. 2002;13(2):71–78. [
PubMed: 11839160]
Bacon O., Chin J., Cohen S. E., et al. Decreased time from human immunodeficiency virus diagnosis to care, antiretroviral therapy initiation, and virologic suppression during the citywide RAPID Initiative in San Francisco.
Clin Infect Dis. 2021;73(1):e122–e128. [
PMC free article: PMC8561247] [
PubMed: 32449916]
Bavinton B. R., Pinto A. N., Phanuphak N., et al. Viral suppression and HIV transmission in serodiscordant male couples: an international, prospective, observational, cohort study.
Lancet HIV. 2018;5(8):e438–e447. [
PubMed: 30025681]
Bellan S. E., Dushoff J., Galvani A. P., et al. Reassessment of HIV-1 acute phase infectivity: accounting for heterogeneity and study design with simulated cohorts.
PLoS Med. 2015;12(3):e1001801. [
PMC free article: PMC4363602] [
PubMed: 25781323]
Benson C., Emond B., Lefebvre P., et al. Rapid initiation of antiretroviral therapy following diagnosis of human immunodeficiency virus among patients with commercial insurance coverage.
J Manag Care Spec Pharm. 2020;26(2):129–141. [
PMC free article: PMC10391294] [
PubMed: 31747358]
Bourgi(a) K., Jenkins C. A., Rebeiro P. F., et al. Weight gain among treatment-naive persons with HIV starting integrase inhibitors compared to non-nucleoside reverse transcriptase inhibitors or protease inhibitors in a large observational cohort in the United States and Canada.
J Int AIDS Soc. 2020;23(4):e25484. [
PMC free article: PMC7159248] [
PubMed: 32294337]
Bourgi(b) K., Rebeiro P. F., Turner M., et al. Greater weight gain in treatment-naive persons starting dolutegravir-based antiretroviral therapy.
Clin Infect Dis. 2020;70(7):1267–1274. [
PMC free article: PMC8205610] [
PubMed: 31100116]
Bruyand M., Thiebaut R., Lawson-Ayayi S., et al. Role of uncontrolled HIV RNA level and immunodeficiency in the occurrence of malignancy in HIV-infected patients during the combination antiretroviral therapy era: Agence Nationale de Recherche sur le Sida (ANRS) CO3 Aquitaine Cohort.
Clin Infect Dis. 2009;49(7):1109–1116. [
PMC free article: PMC2946366] [
PubMed: 19705973]
Buzon M., Siess K., Sone A. Treatment of early HIV infection reduces viral reservoir to levels found in elite controllers. Abstract 151. CROI; 2012 Mar 5-8;
Cain L. E., Logan R., Robins J. M., et al. When to initiate combined antiretroviral therapy to reduce mortality and AIDS-defining illness in HIV-infected persons in developed countries: an observational study.
Ann Intern Med. 2011;154(8):509–515. [
PMC free article: PMC3610527] [
PubMed: 21502648]
Coffey S., Bacchetti P., Sachdev D., et al. RAPID antiretroviral therapy: high virologic suppression rates with immediate antiretroviral therapy initiation in a vulnerable urban clinic population.
AIDS. 2019;33(5):825–832. [
PMC free article: PMC7029629] [
PubMed: 30882490]
Colasanti J., Sumitani J., Mehta C. C., et al. Implementation of a rapid entry program decreases time to viral suppression among vulnerable persons living with HIV in the southern United States.
Open Forum Infect Dis. 2018;5(6):ofy104. [
PMC free article: PMC6022569] [
PubMed: 29992172]
Colfax G. N., Buchbinder S. P., Cornelisse P. G., et al. Sexual risk behaviors and implications for secondary HIV transmission during and after HIV seroconversion.
AIDS. 2002;16(11):1529–1535. [
PubMed: 12131191]
Connor E. M., Sperling R. S., Gelber R., et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group.
N Engl J Med. 1994;331(18):1173–1180. [
PubMed: 7935654]
El-Sadr W. M., Lundgren J., Neaton J. D., et al. CD4+ count-guided interruption of antiretroviral treatment.
N Engl J Med. 2006;355(22):2283–2296. [
PubMed: 17135583]
Ellis R. J., Badiee J., Vaida F., et al. CD4 nadir is a predictor of HIV neurocognitive impairment in the era of combination antiretroviral therapy.
AIDS. 2011;25(14):1747–1751. [
PMC free article: PMC3867631] [
PubMed: 21750419]
Fonner V. A., Denison J., Kennedy C. E., et al. Voluntary counseling and testing (VCT) for changing HIV-related risk behavior in developing countries.
Cochrane Database Syst Rev. 2012;9(9):CD001224. [
PMC free article: PMC3931252] [
PubMed: 22972050]
Friis-Moller N., Thiebaut R., Reiss P., et al. Predicting the risk of cardiovascular disease in HIV-infected patients: the data collection on adverse effects of anti-HIV drugs study.
Eur J Cardiovasc Prev Rehabil. 2010;17(5):491–501. [
PubMed: 20543702]
Garvey L., Surendrakumar V., Winston A. Low rates of neurocognitive impairment are observed in neuro-asymptomatic HIV-infected subjects on effective antiretroviral therapy.
HIV Clin Trials. 2011;12(6):333–338. [
PubMed: 22189152]
Golden M. R., Hogben M., Potterat J. J., et al. HIV partner notification in the United States: a national survey of program coverage and outcomes.
Sex Transm Dis. 2004;31(12):709–712. [
PubMed: 15608584]
Granich R. M., Gilks C. F., Dye C., et al. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model.
Lancet. 2009;373(9657):48–57. [
PubMed: 19038438]
Guay L. A., Musoke P., Fleming T., et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomised trial.
Lancet. 1999;354(9181):795–802. [
PubMed: 10485720]
Guiguet M., Boue F., Cadranel J., et al. Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): a prospective cohort study.
Lancet Oncol. 2009;10(12):1152–1159. [
PubMed: 19818686]
Hare C. B., Pappalardo B. L., Busch M. P., et al. Seroreversion in subjects receiving antiretroviral therapy during acute/early HIV infection.
Clin Infect Dis. 2006;42(5):700–708. [
PubMed: 16447118]
Hecht F. M., Busch M. P., Rawal B., et al. Use of laboratory tests and clinical symptoms for identification of primary HIV infection.
AIDS. 2002;16(8):1119–1129. [
PubMed: 12004270]
Ho J. E., Deeks S. G., Hecht F. M., et al. Initiation of antiretroviral therapy at higher nadir CD4+ T-cell counts is associated with reduced arterial stiffness in HIV-infected individuals.
AIDS. 2010;24(12):1897–1905. [
PMC free article: PMC2903431] [
PubMed: 20543654]
Hocqueloux L., Prazuck T., Avettand-Fenoel V., et al. Long-term immunovirologic control following antiretroviral therapy interruption in patients treated at the time of primary HIV-1 infection.
AIDS. 2010;24(10):1598–1601. [
PubMed: 20549847]
Hollingsworth T. D., Anderson R. M., Fraser C. HIV-1 transmission, by stage of infection.
J Infect Dis. 2008;198(5):687–693. [
PubMed: 18662132]
Hollingsworth T. D., Pilcher C. D., Hecht F. M., et al. High transmissibility during early HIV infection among men who have sex with men-San Francisco, California.
J Infect Dis. 2015;211(11):1757–1760. [
PMC free article: PMC4425938] [
PubMed: 25542958]
Hoy J. F., Grund B., Roediger M., et al. Immediate initiation of antiretroviral therapy for HIV infection accelerates bone loss relative to deferring therapy: findings from the START Bone Mineral Density Substudy, a randomized trial.
J Bone Miner Res. 2017;32(9):1945–1955. [
PMC free article: PMC5555813] [
PubMed: 28650589]
Jain V., Hartogensis W., Bacchetti P., et al. Antiretroviral therapy initiated within 6 months of HIV infection is associated with lower T-cell activation and smaller HIV reservoir size.
J Infect Dis. 2013;208(8):1202–1211. [
PMC free article: PMC3778965] [
PubMed: 23852127]
Kassutto S., Johnston M. N., Rosenberg E. S. Incomplete HIV type 1 antibody evolution and seroreversion in acutely infected individuals treated with early antiretroviral therapy.
Clin Infect Dis. 2005;40(6):868–873. [
PubMed: 15736021]
Koegl C., Wolf E., Hanhoff N., et al. Treatment during primary HIV infection does not lower viral set point but improves CD4 lymphocytes in an observational cohort.
Eur J Med Res. 2009;14(7):277–283. [
PMC free article: PMC3458637] [
PubMed: 19661009]
Koenig S. P., Dorvil N., Dévieux J. G., et al. Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: a randomized unblinded trial.
PLoS Med. 2017;14(7):e1002357. [
PMC free article: PMC5526526] [
PubMed: 28742880]
Kroon Edmb, Phanuphak N., Shattock A. J., et al. Acute HIV infection detection and immediate treatment estimated to reduce transmission by 89% among men who have sex with men in Bangkok.
J Int AIDS Soc. 2017;20(1):21708. [
PMC free article: PMC5515043] [
PubMed: 28691441]
Lafeuillade A., Hittinger G., Lambry V. Long-term control of HIV reservoir after a 2-year ART course at acute infection. Abstract 358. CROI; 2012 Mar 5-8;
Li X., Margolick J. B., Jamieson B. D., et al. CD4+ T-cell counts and plasma HIV-1 RNA levels beyond 5 years of highly active antiretroviral therapy.
J Acquir Immune Defic Syndr. 2011;57(5):421–428. [
PMC free article: PMC3293185] [
PubMed: 21602699]
Li Z., Purcell D. W., Sansom S. L., et al. Vital signs: HIV transmission along the continuum of care - United States, 2016.
MMWR Morb Mortal Wkly Rep. 2019;68(11):267–272. [
PMC free article: PMC6478059] [
PubMed: 30897075]
Lichtenstein K. A., Armon C., Buchacz K., et al. Low CD4+ T cell count is a risk factor for cardiovascular disease events in the HIV outpatient study.
Clin Infect Dis. 2010;51(4):435–447. [
PubMed: 20597691]
Long L. C., Maskew M., Brennan A. T., et al. Initiating antiretroviral therapy for HIV at a patient's first clinic visit: a cost-effectiveness analysis of the rapid initiation of treatment randomized controlled trial.
AIDS. 2017;31(11):1611–1619. [
PMC free article: PMC5512863] [
PubMed: 28463879]
Ma Z. M., Stone M., Piatak M., et al. High specific infectivity of plasma virus from the pre-ramp-up and ramp-up stages of acute simian immunodeficiency virus infection.
J Virol. 2009;83(7):3288–3297. [
PMC free article: PMC2655556] [
PubMed: 19129448]
Manabe Y. C., Campbell J. D., Sydnor E., et al. Immune reconstitution inflammatory syndrome: risk factors and treatment implications.
J Acquir Immune Defic Syndr. 2007;46(4):456–462. [
PubMed: 18077835]
Massanella M., Bender Ignacio R. A., Lama J. R., et al. Long-term effects of early antiretroviral initiation on HIV reservoir markers: a longitudinal analysis of the MERLIN clinical study.
Lancet Microbe. 2021;2(5):e198–e209. [
PubMed: 35544209]
Metsch L. R., Pereyra M., Messinger S., et al. HIV transmission risk behaviors among HIV-infected persons who are successfully linked to care.
Clin Infect Dis. 2008;47(4):577–584. [
PubMed: 18624629]
Mohammed D. Y., Martin E., Brewer R., et al. Same-day medical visit increases viral suppression, Peter Ho Memorial Clinic, 2014-2015 and 2016-2017.
J Assoc Nurses AIDS Care. 2019;30(3):292–300. [
PubMed: 30676360]
Monteiro N., Branco M., Peres S., et al. The impact of tenofovir disoproxil fumarate on kidney function: four-year data from the HIV-infected outpatient cohort.
J Int AIDS Soc. 2014;17(4 Suppl 3):19565. [
PMC free article: PMC4224877] [
PubMed: 25394072]
Nakao J. H., Wiener D. E., Newman D. H., et al. Falling through the cracks? Missed opportunities for earlier HIV diagnosis in a New York City Hospital.
Int J STD AIDS. 2014;25(12):887–893. [
PubMed: 24535693]
O'Connor J., Vjecha M. J., Phillips A. N., et al. Effect of immediate initiation of antiretroviral therapy on risk of severe bacterial infections in HIV-positive people with CD4 cell counts of more than 500 cells per muL: secondary outcome results from a randomised controlled trial.
Lancet HIV. 2017;4(3):e105–e112. [
PMC free article: PMC5337625] [
PubMed: 28063815]
Palella F. J., Hou Q., Li J., et al. Weight gain and metabolic effects in persons With HIV who switch to ART regimens containing integrase inhibitors or tenofovir alafenamide.
J Acquir Immune Defic Syndr. 2023;92(1):67–75. [
PubMed: 36150045]
Pathela P., Jamison K., Braunstein S. L., et al. Initiating antiretroviral treatment for newly diagnosed HIV patients in sexual health clinics greatly improves timeliness of viral suppression.
AIDS. 2021;35(11):1805–1812. [
PubMed: 33973874]
Patterson K. B., Leone P. A., Fiscus S. A., et al. Frequent detection of acute HIV infection in pregnant women.
AIDS. 2007;21(17):2303–2308. [
PubMed: 18090278]
Phanuphak N., Teeratakulpisarn N., van Griensven F., et al. Anogenital HIV RNA in Thai men who have sex with men in Bangkok during acute HIV infection and after randomization to standard vs. intensified antiretroviral regimens.
J Int AIDS Soc. 2015;18(1):19470. [
PMC free article: PMC4425809] [
PubMed: 25956171]
Pilcher C. D., Ospina-Norvell C., Dasgupta A., et al. The effect of same-day observed initiation of antiretroviral therapy on HIV viral load and treatment outcomes in a US public health setting.
J Acquir Immune Defic Syndr. 2017;74(1):44–51. [
PMC free article: PMC5140684] [
PubMed: 27434707]
Pilcher C. D., Tien H. C., Eron J. J., et al. Brief but efficient: acute HIV infection and the sexual transmission of HIV.
J Infect Dis. 2004;189(10):1785–1792. [
PubMed: 15122514]
Pires A., Hardy G., Gazzard B., et al. Initiation of antiretroviral therapy during recent HIV-1 infection results in lower residual viral reservoirs.
J Acquir Immune Defic Syndr. 2004;36(3):783–790. [
PubMed: 15213561]
Prevention Access Campaign. Prevention Access Campaign consensus statement: risk of sexual transmission of HIV from a person living with HIV who has an undetectable viral load. 2018.
https://www.preventionaccess.org/consensus [accessed 2018 Aug 21]
Quinn T. C., Wawer M. J., Sewankambo N., et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group.
N Engl J Med. 2000;342(13):921–929. [
PubMed: 10738050]
Rodger A. J., Cambiano V., Bruun T., et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study.
Lancet. 2019;393(10189):2428–2438. [
PMC free article: PMC6584382] [
PubMed: 31056293]
Rodger A. J., Cambiano V., Bruun T., et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner Is using suppressive antiretroviral therapy.
JAMA. 2016;316(2):171–181. [
PubMed: 27404185]
Rosen(a) S., Maskew M., Fox M. P., et al. Initiating antiretroviral therapy for HIV at a patient's first clinic visit: the RapIT randomized controlled trial.
PLoS Med. 2016;13(5):e1002015. [
PMC free article: PMC4862681] [
PubMed: 27163694]
Rosen(b) S., Maskew M., Fox M. P., et al. Correction: Initiating antiretroviral therapy for HIV at a patient's first clinic visit: the RapIT randomized controlled trial.
PLoS Med. 2016;13(6):e1002050. [
PMC free article: PMC4892484] [
PubMed: 27258028]
Rutstein S. E., Ananworanich J., Fidler S., et al. Clinical and public health implications of acute and early HIV detection and treatment: a scoping review.
J Int AIDS Soc. 2017;20(1):21579. [
PMC free article: PMC5515019] [
PubMed: 28691435]
Sabin C. A., Smith C. J., d'Arminio Monforte A., et al. Response to combination antiretroviral therapy: variation by age.
AIDS. 2008;22(12):1463–1473. [
PubMed: 18614870]
Saez-Cirion A., Bacchus C., Hocqueloux L., et al. Post-treatment HIV-1 controllers with a long-term virological remission after the interruption of early initiated antiretroviral therapy ANRS VISCONTI Study.
PLoS Pathog. 2013;9(3):e1003211. [
PMC free article: PMC3597518] [
PubMed: 23516360]
Scherrer A. U., von Wyl V., Yang W. L., et al. Emergence of acquired HIV-1 drug resistance almost stopped in Switzerland: a 15-year prospective cohort analysis.
Clin Infect Dis. 2016;62(10):1310–1317. [
PubMed: 26962075]
Siddiqi A. E., Hall H. I., Hu X., et al. Population-based estimates of life expectancy after HIV diagnosis: United States 2008-2011.
J Acquir Immune Defic Syndr. 2016;72(2):230–236. [
PMC free article: PMC4876430] [
PubMed: 26890283]
Silverberg M. J., Chao C., Leyden W. A., et al. HIV infection, immunodeficiency, viral replication, and the risk of cancer.
Cancer Epidemiol Biomarkers Prev. 2011;20(12):2551–2559. [
PMC free article: PMC3237725] [
PubMed: 22109347]
Skarbinski J., Rosenberg E., Paz-Bailey G., et al. Human immunodeficiency virus transmission at each step of the care continuum in the United States.
JAMA Intern Med. 2015;175(4):588–596. [
PubMed: 25706928]
Stekler J. D., Violette L. R., Niemann L. A., et al. Seroconversion, seroreversion, and serowaffling among participants initiating antiretroviral therapy in Project DETECT.
Int J STD AIDS. 2023;34(6):385–394. [
PubMed: 36703607]
Steward W. T., Remien R. H., Higgins J. A., et al. Behavior change following diagnosis with acute/early HIV infection-a move to serosorting with other HIV-infected individuals. The NIMH Multisite Acute HIV Infection Study: III.
AIDS Behav. 2009;13(6):1054–1060. [
PMC free article: PMC2785897] [
PubMed: 19504178]
Streeck H., Jessen H., Alter G., et al. Immunological and virological impact of highly active antiretroviral therapy initiated during acute HIV-1 infection.
J Infect Dis. 2006;194(6):734–739. [
PubMed: 16941338]
Torok M. E., Yen N. T., Chau T. T., et al. Timing of initiation of antiretroviral therapy in human immunodeficiency virus (HIV)--associated tuberculous meningitis.
Clin Infect Dis. 2011;52(11):1374–1383. [
PMC free article: PMC4340579] [
PubMed: 21596680]
Tozzi V., Balestra P., Bellagamba R., et al. Persistence of neuropsychologic deficits despite long-term highly active antiretroviral therapy in patients with HIV-related neurocognitive impairment: prevalence and risk factors.
J Acquir Immune Defic Syndr. 2007;45(2):174–182. [
PubMed: 17356465]
van Lelyveld S. F., Gras L., Kesselring A., et al. Long-term complications in patients with poor immunological recovery despite virological successful HAART in Dutch ATHENA cohort.
AIDS. 2012;26(4):465–474. [
PubMed: 22112603]
Verburgh M. L., Wit F. W., Boyd A., et al. One in 10 virally suppressed persons with HIV in The Netherlands experiences >/=10% weight gain after switching to tenofovir alafenamide and/or integrase strand transfer inhibitor.
Open Forum Infect Dis. 2022;9(7):ofac291. [
PMC free article: PMC9301581] [
PubMed: 35873291]
Winston A., Puls R., Kerr S. J., et al. Dynamics of cognitive change in HIV-infected individuals commencing three different initial antiretroviral regimens: a randomized, controlled study.
HIV Med. 2012;13(4):245–251. [
PubMed: 22151608]
Wright S. T., Carr A., Woolley I., et al. CD4 cell responses to combination antiretroviral therapy in patients starting therapy at high CD4 cell counts.
J Acquir Immune Defic Syndr. 2011;58(1):72–79. [
PMC free article: PMC3159689] [
PubMed: 21654498]
Wu Z., Zhao Y., Ge X., et al. Simplified HIV testing and treatment in China: analysis of mortality rates before and after a structural intervention.
PLoS Med. 2015;12(9):e1001874. [
PMC free article: PMC4562716] [
PubMed: 26348214]
Xia Q., Maduro G. A., Li W., et al. Life expectancy among people with HIV in New York City, 2009-2018.
J Acquir Immune Defic Syndr. 2022;91(5):434–438. [
PubMed: 36084201]
Young J., Psichogiou M., Meyer L., et al. CD4 cell count and the risk of AIDS or death in HIV-Infected adults on combination antiretroviral therapy with a suppressed viral load: a longitudinal cohort study from COHERE.
PLoS Med. 2012;9(3):e1001194. [
PMC free article: PMC3308938] [
PubMed: 22448150]
Zolopa A., Andersen J., Powderly W., et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial.
PLoS One. 2009;4(5):e5575. [
PMC free article: PMC2680972] [
PubMed: 19440326]
Zulliger R., Black S., Holtgrave D. R., et al. Cost-effectiveness of a package of interventions for expedited antiretroviral therapy initiation during pregnancy in Cape Town, South Africa.
AIDS Behav. 2014;18(4):697–705. [
PMC free article: PMC3984926] [
PubMed: 24122044]
Conflict of Interest: There are no author or writing group conflict of interest disclosures.
Created: August 2018; Last Update: July 2021.
![Figure 1. HIV Test Window of Detection [a,b].](/books/NBK563020/bin/nycgacute-Image001.jpg)