| Treatmentrelated mortality | 0 per 1000 | 0 per 1000
(0 to 0) | RR 2.88
(0.12 to 69.16) | 100
(1 study) | ⊕⊝⊝⊝
very low1,2 | |
| Overall Survival | Study population | HR 1
(0.75 to 1.31) | 247
(3 studies) | ⊕⊝⊝⊝
very low1,4,5,9,13,21,22 | |
| See comment3 | See comment3 |
| Moderate |
| 0 per 10003 | -214748364
8 per 1000
(-2147483648 to -2147483648)3 |
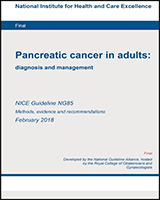
| Time to stent dysfunction for unresectable PC - primary and/or secondary stent | Study population | HR 2.59
(1.67 to 4) | 229
(3 studies) | ⊕⊝⊝⊝
very low3,4,5,8,9,13,17,18 | |
| See comment3 | See comment3 |
| Moderate |
| 0 per 10003 | -214748364
8 per 1000
(-2147483648 to -2147483648)3 |
| Time to stent dysfunction for unresectable PC - Covered or Partially Covered SEMS (Primary Stent only) | 257 per 1000 | 489 per 1000
(350 to 649) | HR 2.26
(1.45 to 3.53) | 224
(2 studies) | ⊕⊝⊝⊝
very low4,5,6,7,8 | |
| Time to stent dysfunction for unresectable PC - Uncovered SEMS (Primary Stent only) | 167 per 1000 | 421 per 1000
(232 to 677) | HR 3
(1.45 to 6.2) | 117
(1 study) | ⊕⊝⊝⊝
very low4,6,7,8 | |
| Time to stent dysfunction for unresectable PC - Partially Covered SEMS (Secondary Stent only) | 118 per 1000 | 567 per 1000
(160 to 982) | HR 6.69
(1.39 to 32.07) | 33
(1 study) | ⊕⊝⊝⊝
very low4,6,7,8 | |
| Time to stent dysfunction for unresectable PC - Uncovered SEMS (Secondary Stent only) | 67 per 1000 | 497 per 1000
(212 to 862) | HR 9.97
(3.46 to 28.74) | 31
(1 study) | ⊕⊝⊝⊝
very low4,6,7,8 | |
| Stent Dysfunction - Stent Occlusion | 191 per 1000 | 430 per 1000
(319 to 577) | RR 2.25
(1.67 to 3.02) | 471
(6 studies) | ⊕⊕⊝⊝
low1,4,5,9,10,11,12,13,14,15 | |
| Stent Dysfunction - Stent Migration | 91 per 1000 | 17 per 1000
(2 to 143) | RR 0.19
(0.02 to 1.57) | 113
(1 study) | ⊕⊝⊝⊝
very low2,4,5 | |
| Stent Dysfunction - Stent Occlusion or Migration | 167 per 1000 | 403 per 1000
(240 to 677) | RR 2.42
(1.44 to 4.06) | 171
(1 study) | ⊕⊝⊝⊝
very low4,6,7,8 | |
| Stent Occlusion - any type of SEMS | 176 per 1000 | 387 per 1000
(255 to 590) | RR 2.2
(1.45 to 3.35) | 258
(4 studies) | ⊕⊝⊝⊝
very low4,8,9,10,11,12,13,14,15 | |
| Stent Occlusion - Covered SEMS | 212 per 1000 | 487 per 1000
(319 to 738) | RR 2.3
(1.51 to 3.49) | 213
(2 studies) | ⊕⊝⊝⊝
very low1,4,5,8 | |
| Stent Occlusion - unresectable patients | 174 per 1000 | 410 per 1000
(295 to 570) | RR 2.36
(1.7 to 3.28) | 417
(5 studies) | ⊕⊕⊝⊝
low1,4,5,9,11,12,13,14 | |
| Stent Occlusion - resectable, borderline resectable or locally advanced | 303 per 1000 | 524 per 1000
(270 to 1000) | RR 1.73
(0.89 to 3.34) | 54
(1 study) | ⊕⊕⊝⊝
low4,10,15,16 | |
| Pancreatitis | 22 per 1000 | 18 per 1000
(7 to 46) | RR 0.81
(0.32 to 2.04) | 720
(7 studies) | ⊕⊝⊝⊝
very low1,2,4,5,6,9,10,11,13,14,15,17 | |
| Pancreatitis - any SEMS | 25 per 1000 | 26 per 1000
(9 to 73) | RR 1.02
(0.36 to 2.92) | 473
(4 studies) | ⊕⊝⊝⊝
very low2,4,6,7,10,11,14,15,17,18 | |
| Pancreatitis - covered SEMS | 19 per 1000 | 6 per 1000
(1 to 58) | RR 0.32
(0.03 to 3.01) | 213
(2 studies) | ⊕⊝⊝⊝
very low1,2,4,5 | |
| Pancreatitis - unresectable patients | 1 per 100 | 1 per 100
(0 to 4) | RR 1.52
(0.51 to 4.59) | 632
(5 studies) | ⊕⊝⊝⊝
very low1,2,4,5,6,7,9,11,14,17,18 | |
| Pancreatitis - resectable, borderline resectable or locally advanced patients | 182 per 1000 | 22 per 1000
(2 to 365) | RR 0.12
(0.01 to 2.01) | 54
(1 study) | ⊕⊝⊝⊝
very low2,4,10,15 | |
| Cholangitis - unresectable patients | 30 per 1000 | 93 per 1000
(38 to 224) | RR 3.1
(1.28 to 7.48) | 334
(4 studies) | ⊕⊕⊝⊝
low1,4,9,11,13,17,18 | |
| Cholangitis - any SEMS | 39 per 1000 | 67 per 1000
(19 to 229) | RR 1.71
(0.5 to 5.89) | 152
(2 studies) | ⊕⊝⊝⊝
very low2,4,9,11,13,14 | |
| Cholangitis - covered SEMS | 0 per 1000 | 0 per 1000
(0 to 0) | RR 4.81
(0.24 to 97.68) | 100
(1 study) | ⊕⊝⊝⊝
very low1,2 | |
| Cholangitis - partiallycovered SEMS | 49 per 1000 | 244 per 1000
(57 to 1000) | RR 5
(1.17 to 21.43) | 82
(1 study) | ⊕⊝⊝⊝
very low4,16,17,18 | |
| Cholecystitis -unresectable patients | 27 per 1000 | 13 per 1000
(4 to 41) | RR 0.47
(0.15 to 1.53) | 448
(4 studies) | ⊕⊝⊝⊝
very low2,4,5,6,7,9,13,17,18 | |
| Cholecystitis - any SEMS | 6 per 1000 | 16 per 1000
(2 to 123) | RR 2.56
(0.33 to 20.1) | 253
(2 studies) | ⊕⊝⊝⊝
very low2,4,6,7,9,13 | |
| Cholecystitis - partiallycovered SEMS | 49 per 1000 | 10 per 1000
(0 to 197) | RR 0.2
(0.01 to 4.04) | 82
(1 study) | ⊕⊝⊝⊝
very low2,4,17,18 | |
| Cholecystitis - Covered SEMS | 73 per 1000 | 8 per 1000
(1 to 139) | RR 0.11
(0.01 to 1.91) | 113
(1 study) | ⊕⊝⊝⊝
very low2,4,5 | |
| # patients with cholestatic symptoms to 2- FU Follow-up: 2 years | 250 per 1000 | 360 per 1000
(183 to 710) | RR 1.44
(0.73 to 2.84) | 79
(1 study) | ⊕⊝⊝⊝
very low2,4,17,18 | |
| Post-ES Haemorrhage | Study population | RR 3
(0.12 to 72.18) | 118
(1 study) | ⊕⊝⊝⊝
very low2,4,11,14 | |
| 0 per 1000 | 0 per 1000
(0 to 0) |
| Moderate |
| 0 per 1000 | 0 per 1000
(0 to 0) |
| Hospitalisation Days | | The mean hospitalisati on in the intervention groups was
0.49 standard deviations higher
(0.21 to 0.77 higher) | | 197
(2 studies) | ⊕⊝⊝⊝
very low4,11,14,16,17,18 | |
| # >=30% decrease in serum bilirubin | 1000 per 1000 | 940 per 1000
(790 to 1000) | RR 0.94
(0.79 to 1.1) | 34
(1 study) | ⊕⊕⊝⊝
low9,16 | |
| % Reduction in total serum bilirubin levels | The mean % reduction in total serum bilirubin levels in the control groups was
74 percent age | The mean % reduction in total serum bilirubin levels in the intervention groups was
10.3 lower
(32.51 lower to 11.91 higher) | | 79
(1 study) | ⊕⊝⊝⊝
very low4,17,18,19,20 | |
| Total Serum Bilirubin - rate of change | | The mean total serum bilirubin - rate of change in the intervention groups was
0.23 standard deviations lower
(0.62 lower to 0.17 higher) | | 98
(1 study) | ⊕⊕⊝⊝
low1,16 | |